The most preventable form of human pain is that inflicted in the form of torture
– World Medical Association
Pain is a universal human experience, however each human experiences pain uniquely.
So, when I was asked to team with Psychiatrist, Sarah Acland, MD, to talk about pain management for survivors of torture, I thought I could cover the topic well by simply falling back on the standard approach I’ve used in treating all my patients with chronic pain – a BIO-PSYCHO-SOCIAL approach.
But as I researched more about the profound struggles survivors of torture face, I began to question whether or not another approach was necessary for this group of patents.
In the end, I returned to the realization that a (1) biological + (2) psychological + (3) sociological approach is well-suited to care for the survivors of torture, as long as caregivers are thorough in evaluating, understanding, and optimizing each of the three elements.
Pain is defined as: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage (IASP)
Pain is a necessary body system that, while unpleasant, protects us from harm. But in survivors of torture, this “useful pain” can be hijacked by a damaged nervous system, heard through the amplified megaphone of psychological distress, and experienced in a prison of cultural barriers.
To understand how best to help these survivors, one must have some understanding of how the body’s pain system is wired. It’s not as simple as two points connected by a nerve. When trauma is inflicted, pain receptors transmit multiple nerve impulses toward the brain (i.e. the “ascending” pathways). These sensory impulses travel up different tracks at different speeds to not just one, but to several areas of the brain – both “conscious” and “unconscious.” At the same time, the nervous system will try to dampen (“modulate”) the ascending pain impulses by releasing chemicals and sending impulses downward (i.e. the “descending” pathways).
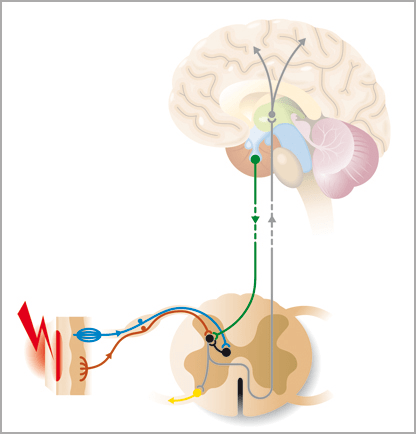
Granted, my explanation grossly oversimplifies the complex interactions between the ascending (pain) and descending (anti-pain) pathways, but it lays the foundation for understanding how we can treat pain.
Use treatments that (a) enhance the descending anti-pain pathways, such as:
- Some antidepressants
- Endorphins (exercise)
- Physical therapy/occupational therapy
- Psychotherapy
And (b) treatments that dampen the ascending painful pathways:
- Physical medicine (e.g., ice/heat)
- NSAIDs
- Stimulators (e.g. TENS)
- Some anti-epileptics (e.g., gabapentin)
- Nerve blocks
- Opioids
As Bing would say… You have to accentuate the positive and eliminate the negative.

Effective treatment also depends upon knowing the degree to which the pain is nociceptive (“normal”) or neuropathic (“abnormal”).
Types of Pain (IASP)
Nociceptive pain occurs when diseased or traumatized tissue activates the nervous system and its receptors (i.e. nociceptors). On the other hand, neuropathic pain is when disease or trauma (i.e. pathology) to the nervous system itself causes pain. Nociceptive pain is usually sharp, acute, and localized. Neuropathic pain is usually dull, burning, aching, chronic, and poorly localized. Nociceptive pain is usually associated with defined tissue damage. Neuropathic pain can persist long after the traumatized tissue has healed and there are no physical findings.
To varying degrees, all pain syndromes (acute and chronic) have some combination of both neuropathic and nociceptive pain. Neuropathic pain is actually the most prevalent type of pain in developing nations and prominently results from torture. Neuropathic pain is difficult to cure, and generally must be “managed” with measures to augment activity in descending modulating pain pathways.
By design, torture often doesn’t physically “leave a mark” after the acute injuries have healed. Most common is blunt trauma, especially to soles of feet (“falanga”), often leading to chronic neuropathic pain.
Also common is suspension of the body, i.e. stretching nerves, leading to musculoskeletal joint/soft tissue damage and “plexopathy.”
Regardless of the physical signs left by torture, the marks left by psychological trauma is nearly universal, i.e., PTSD.
Obviously, my presentation to this point has primarily focused on biological (i.e., physical) aspects of pain and pain treatment. The psychological and social aspects are equally important, but are beyond the scope of this brief overview. Suffice it to say, effective pain care requires a team approach (i.e., multidisciplinary). Mental health issues (e.g., PTSD, depression, anxiety) almost always co-exist with chronic pain and lead to, or are influenced by, social/family/cultural circumstances. The following lists offer some insight into just how challenging it can be to treat pain in survivors of torture.
Treatment barriers to overcome include:
- Language/communication
- Cultural barriers
- Memories of helplessness fear & shame
- Impaired recollection
- Survivors may not offer information unless asked
- Non-compliance with treatment
- Reticent to use meds due to past forced use
Findings suggestive of torture:
- Multiple chronic pains
- Multiple physical scars
- Complex injuries
- Musculoskeletal pain
- Headaches
- Neuritis
- Depression
- Anxiety
- PTSD
- Neuropathic pain
Effective treatment augmented by:
– Trust and communication
– Evaluate in a calm atmosphere
– Be thorough
– Offer detailed explanations
– Obtain informed consent
– Allow the patient to have control
– Minimize exhaustive visits for tests & specialists
– Identify potentially treatable disorders
– Ask patients about their beliefs about the pain
(e.g., Pain may be assumed to signal ongoing damage)
– Set realistic and clear goals/expectations
– Stepwise approach to treatment
– Avoid reinforcing/addictive drugs
– Injections might trigger flashbacks
Summary:
In all individuals, to varying degrees, pain has biological, psychological & sociological elements. All three elements feature prominently in torture survivors. Effective treatment must address all three (i.e., a bio-psycho-social treatment model), and is best achieved by using a multidisciplinary approach (i.e., psychotherapy, physical medicine & traditional clinical medicine). Establishing trust and effective communication can be challenging but is crucial.
Pain can be effectively managed in survivors of torture in the same thorough step-wise manner used to treat other patients as long as caregivers work as a team to fully address all three elements in the bio-psycho-social treatment model.
Another final point, among the many, I took away from this interactive presentation with my colleagues on that April Friday morning was this one I initially took for granted, but was so eloquently emphasized by Dr. Acland… That they are victims cannot be overlooked, but that they are survivors can never be forgotten.
Pain has an element of blank;
It cannot recollect
When it began, or if there were
A day when it was not.
– Emily Dickinson

Pain Management:
Implications for Caring for Refugee & Immigrant Survivors of Torture
Survivors of Torture Recovery Center
Kent School of Social Work
University of Louisville
April 8, 2016
James Patrick Murphy, MD, MMM

*
*
*