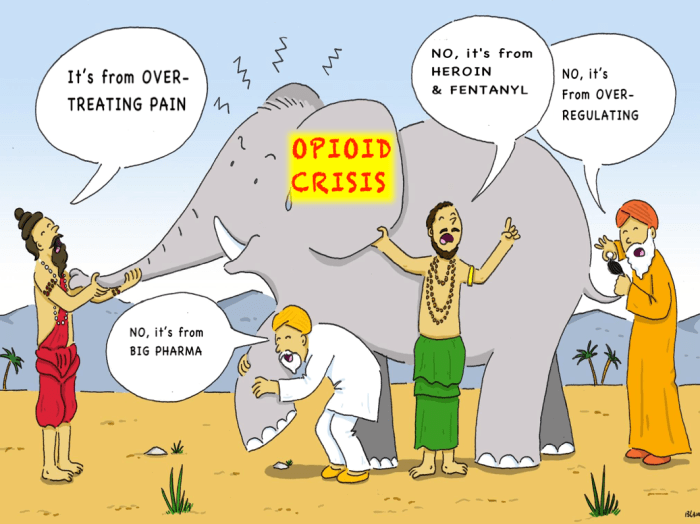
There is an Indian fable about a group of blind wise men asked to describe an elephant. Each felt only the part of the pachyderm closest to him and thus came up with vastly different truths as to what an elephant is.
Our country has an elephant in our room and it’s called the OPIOID CRISIS. And many of our wise men and women are trying very hard to slay this colossus. Sadly, like the blind men in the fable, they often take aim at only what’s in front of them, missing the heart of the matter and making the beast more angry.
For many, the opioid crisis is primarily perceived as a prescribing problem. Thus, their weapon of choice is PAIN REGULATIONS.
One example of this is House Bill 333, passed this summer by Kentucky’s legislature and later turned into regulations by the Kentucky Board of Medical Licensure on November 15, 2017. These new regulations are have been advertised as (a) merely imposing a three-day limit on prescribing controlled substances for acute pain, because (b) the CDC Guideline demands it. In fact, the clearly voluntary CDC Guideline falls way short of demanding anything…
…And the new Kentucky regulations dictate more than has been advertised.
Even before House Bill 333 came along, embedded in the many pages of Kentucky pain regulations was this dictum:
“The physician shall discontinue controlled substance treatment or refer the patient to addiction management if: There has been no improvement in function and response to the medical complaint and related symptoms, if improvement is medically expected.”
And, as pointed out earlier, Kentucky physicians have been led to believe that the only new regulation is a three-day limit on prescribing schedule two controlled substances to treat acute pain. But there’s more. Much more.
For starters, Kentucky has added a new definition of “high risk” regimens: “dosages greater than or equal to fifty (50) MME/day or opioids with benzodiazepines, without evidence of benefit.” (MME = morphine milligram equivalent)
Now, going forward if a patient meets these criteria…
Or: “Controlled substance therapy has produced significant adverse effects, including instances such as an overdose or events leading to hospitalization or disability”
Or: “The patient exhibits inappropriate drug-seeking behavior or diversion”
Then the physician shall “taper controlled substances.”
But wait, you can’t just taper someone anyway you want to anymore. Now you must taper the medications “in a manner slow enough to minimize symptoms and signs of opioid withdrawal.”
And, hold on, we aren’t done with these new tapering regulations yet. While you are slowly and carefully tapering you must also, “Collaborate with other specialists as needed to optimize nonopioid pain management and psychosocial support for anxiety related to the taper.”
So, let’s review what you have learned about this new regulatory elephant gun:
(1) We are now prohibited (with some exceptions) from giving more than three days of schedule two meds for acute pain.
(2) We’d better find a way to adequately document that there is benefit to our “high risk” regimens.
(3) If virtually anything goes awry, we now must taper very carefully (and with the help of specialists to relieve the patient’s anxiety) to minimize withdrawal symptoms.
(4) And I have failed to mention that, inexplicably, there is now the requirement that a physician “shall stop prescribing or dispensing any controlled substance taken less frequently than once a day.” So if you are somehow able to get your patient to take less pain medication, and it becomes needed less frequently than everyday, your wonderful patient gets rewarded by you having to stop prescribing pain meds altogether? Seriously, what part of the elephant were they feeling when they wrote that regulation?
In conclusion, my purpose in writing this article is not to be overly critical of the well-meaning people who write our regulations. I simply want my colleagues in Kentucky to know that there is much more to the opioid crisis elephant than simply the prescribing component and much more to Kentucky’s new pain regulations than just a limit on acute pain meds. Please don’t get trampled.
Disclaimer: This is not medical or legal advice. This is my personal opinion. Please read the regulations yourself and get a lawyer if you want legal advice.
References:
Indian fable:https://wildequus.org/2014/05/07/sufi-story-blind-men-elephant
OpioidCrisis:https://www.cdc.gov/drugoverdose/epidemic/index.html
CDCGuideline:https://www.cdc.gov/mmwr/volumes/65/rr/rr6501e1.htm
KBML Pain Regs:https://kbml.ky.gov/board/Pages/krs-amendment.aspx
*This is Water. Commencement Speech to Kenyon College class of 2005 written by David Foster Wallace: https://www.youtube.com/watch?v=8CrOL-ydFMI
*
*
*
