Please take three minutes to read how you can help a small committee make a BIG impact in the lives of Kentuckians battling opioid addiction.
Buprenorphine — a safe and effective medication for the treatment of opioid use disorder (MOUD) — is vital to reducing overdose deaths. Yet Kentuckians’ access to this lifesaving medication is in jeopardy because of an outdated, ten-year-old regulation still on the books: 201 KAR 9:270.
But there’s hope.
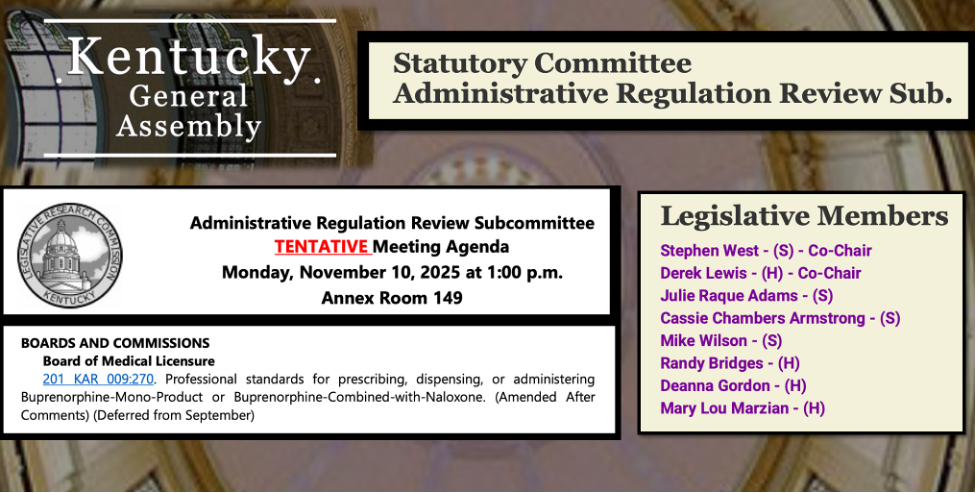
On November 10, 2025, the Administrative Regulation Review Subcommittee (ARRS) of Kentucky’s General Assembly has the power to reject the Kentucky Board of Medical Licensure’s (KBML) flawed update to this harmful rule.
Why the KBML Proposal Must Be Rejected
The KBML’s proposed update to 201 KAR 9:270 is insufficient, critically flawed, and should be sent back for comprehensive revision — or better yet, repealed altogether.
At its heart, this is about access.
Kentuckians battling opioid addiction need fewer barriers to buprenorphine, not more. Yet this regulation does the opposite — it’s full of unnecessary restrictions that are:
- Outdated
- Unsupported by research
- Condemned by experts
- Punitive toward people with addiction
Four Truths Everyone Should Know
1. Buprenorphine works.
The Kentucky Opioid Response Effort (KORE) reports that buprenorphine (and methadone) reduce illicit drug use and fatal overdose by over 50% — and improve quality of life.
If you would like to know more about how buprenorphine works to save lives, please check out this recent KET special:
🎥 Managing the Disease of Addiction (KET Kentucky Health)

2. Kentucky needs fewer barriers.
The Federation of State Medical Boards — of which Kentucky is a member — says that “reducing barriers to treatment” with buprenorphine is critical to “decreasing the risk of overdose.”
3. 201 KAR 9:270 is a proven barrier.
A recent study by Kentucky researchers repeatedly cited this KBML regulation as a barrier preventing people from receiving lifesaving treatment.
4. The ARRS has rejected KBML proposals before.
In 2008, after ARRS pushed back, KBML admitted in its fall newsletter:
“Acting on a request of the Kentucky General Assembly’s Administrative Review Subcommittee (ARRS), the Board has agreed to withdraw all of its existing guidelines.”
The Correct Course Is Clear
Reject 201 KAR 9:270.
On November 10, the ARRS can send this regulation back to KBML and direct them to work collaboratively with Kentucky’s addiction medicine specialists and other experts to create evidence-based, compassionate policy that expands access to treatment rather than restricting it.
What You Can Do
You’ve already taken the first step by reading this article. Thank you.
If you want to make your voice heard, contact ARRS members today and urge them to reject KBML’s proposed update to 201 KAR 9:270.
📞 Phone: 502-564-8100
Email ARRS Members:
- Stephen West (S) – Co-Chair: steve.west@kylegislature.gov
- Derek Lewis (H) – Co-Chair: Derek.Lewis@kylegislature.gov
- Julie Raque Adams (S): julie.adams@kylegislature.gov
- Cassie Chambers Armstrong (S): cassie.armstrong@kylegislature.gov
- Mike Wilson (S): mike.wilson@kylegislature.gov
- Randy Bridges (H): randy.bridges@kylegislature.gov
- Deanna Gordon (H): deanna.gordon@kylegislature.gov
- Mary Lou Marzian (H): marylou.marzian@kylegislature.gov
This issue has flown under the radar for far too long. Now that you know, please help get this outdated regulation off the books.
And if you can, join us in Frankfort on November 10 for the ARRS meeting — it’s open to the public. Maybe I’ll see you there.
In hope for a better future for Kentucky,
James Patrick Murphy, MD
