Buprenorphine is an FDA-approved medication for treating opioid use disorder, proven to be effective inpreventingoverdose deaths, reducing drug related crime, recidivism, and drug diversion, while saving valuable community resources.
However, Kentucky’s buprenorphine prescribing regulation 201 KAR 9:270 is outdated, unnecessary and harmful, because it creates barriers to accessing this lifesaving care.
Furthermore, despite all good intentions, this regulation paradoxically increases crime and diversion. Thus, for the safety of our communities, 201 KAR 9:270 must be repealed.
• Despite law enforcement, DEA, policy-makers, and medical experts universally calling for the removal of barriers to accessing buprenorphine, barriers continue to exist, e.g., stigma, costs, irrational fear of diversion, prescriber trepidation, and pharmacist and prescriber fear of regulatory scrutiny. 201 KAR 9:270 contributes to all of these barriers.
• 201 KAR 9:270 is a barrier to buprenorphine treatment, because it rigidly mandates actions that should be dependent on individual patient circumstances and prescriber clinical judgment; actions such as: frequent in-person evaluations, mandatory specialist consults, numerous urine drug tests, extensive labs, psychological counseling, outdated dosage limits, and irrational limits on medications for co-occurring conditions. Laws mandating such measures are not supported by scientific evidence, federal policies, or clinical practice guidelines from the American Society of Addiction Medicine.
• Frankly, Kentucky’s buprenorphine law 201 KAR 9:270 is years behind the times. To illustrate just how absurd it has become, consider that Kentucky requires a special DEA “X-Waiver” that doesn’t even exist anymore. On December 29, 2022, in an effort to increase access to buprenorphine, Congress eliminated all buprenorphine-specific federal regulations, e.g., the DEA “X-Waiver,” along with caps on the number of patients per prescriber, prescriber limits, mandated education. But 201 KAR 9:270 still requires prescribers to have the “X-Waiver.”
• In sum, Kentucky has perhaps the most outdated, draconian, and harmful buprenorphine regulation in our nation and is one of only 19 states that still have buprenorphine-specific regulations on their books. And sadly, prescriptions for buprenorphine in Kentucky have only decreased at a time when overdose rates are still at record levels. Repealing 201 KAR 9:270 is common sense.
Why is this so?
Because of rapidly evolving scientific and clinical knowledge, it’s impossible for policymakers to create regulations that strictly tell clinicians how to treat addiction with buprenorphine. Beyond that, Kentucky’s deliberate regulatory process is too slow and renders obsolete any attempt at reworking 201 KAR 9:270 even before the ink dries on the page.
Therefore, to save lives, reduce crime, and improve the health and well-being of our communities, please join the Kentucky Society of Addiction Medicine and support repeal of Kentucky’s buprenorphine regulation 201 KAR 9:270. This decade old law is outdated, unfixable, unnecessary, and harms the people it was intended to help. It mandates actions that are not supported by evidence, actions that inhibit access to treatment, actions that lead to increase drug related crime, and actions that promote fraud, waste, and abuse.
Rather than discourage drug diversion, 201 KAR 9:270 actually worsens drug related crime and diversion. And tragically, Kentuckians struggling with addiction are needlessly dying because of barriers to treatment caused by this law.
Repeal of 201 KAR 9:270 would allow buprenorphine to assume its rightful place in the category of DEA Schedule III medications with low risk, allowing clinicians to prescribe buprenorphine for its legitimate medical purpose in the usual course of sound professional practice. Make our communities safer and healthier. Repeal of 201 KAR 9:270 is critically necessary.
A summation of clinical, social, and scientific evidence, as well as expert opinion and federal policy focusing on DIVERSION, CRIME, and ACCESS:
Treatment with buprenorphine was associated with a REDUCTION IN ARRESTS, via Addiction Medicine, the official journal of ASAM. https://pubmed.ncbi.nlm.nih.gov/30916463/
Any steps taken to minimize buprenorphine DIVERSION and misuse must be careful not to undermine the positive patient and public health benefits gained from expanded treatment access, via University of Kentucky. https://pubmed.ncbi.nlm.nih.gov/25221984/
Barriers to treatment with buprenorphine include “Aggressive enforcement strategies by the DEA and several state attorneys general—including increases in raiding, auditing, and launching criminal investigations of waivered providers,” via National Academies of Science.https://nap.nationalacademies.org/read/25310/chapter/7#120
The Kentucky Medical Association (KMA), American Medical Association, and the American Society of Addiction Medicine (ASAM) support a bill (House Bill 121) that would remove insurance barriers to treatment with buprenorphine. The rationale supporting House Bill 121 (noted below) also supports the Kentucky Society of Addiction Medicine’s call for repeal of 201 KAR 9:270. For context, I encourage you to read the following “one-page” support document from the AMA:
For more information, please go to my blog CONFLUENTIAL TRUTH https://jamespmurphymd.com and start scrolling. Related stories begin with my post on June 28, 2024 about a petition to the Kentucky Board of Medical Licensure…
Buprenorphine is a safe, effective, and life-saving medication for the treatment of people with opioid use disorder. However, due to buprenorphine access barriers, such as Kentucky’s buprenorphine regulation (201 KAR 9:270), buprenorphine is accessed by only approximately one out of five people who need treatment with this medication. 201 KAR 9:270 limits access to life-saving treatment with buprenorphine, worsens the societal impact of the opioid crisis, perpetuates stigma, and harms the people it was intended to help. Considering current scientific evidence, there is no plausible reason a separate buprenorphine-specific regulation, like 201 KAR 9:270, should continue to exist in Kentucky, especially considering our federal government has eliminated more restrictive national buprenorphine-specific regulations.
Recently, I was invited to testify in Kentucky’s capital on behalf of my Kentucky Society of Addiction Medicine colleagues regarding KY’s outdated buprenorphine regulation. My televised address to the Kentucky General Assembly’s Interim Joint Committee on Health Services on October 23, 2024 focused on six good reasons 201 KAR 9:270 needs to be repealed.
In truth, working together we can dramatically lower the opioid overdose rate in Kentucky and save thousands of lives each year. But a major barrier standing in our way is Kentucky’s outdated regulation (201 KAR 9:270) that restricts how physicians prescribe buprenorphine to treat patients with the disease of opioid use disorder.
I urge you to learn more about how experts, advocates, and concerned citizens are working to remove this harmful barrier to lifesaving care, by clicking on the links provided below:
So, if you’ve read this far, first of all, THANK YOU! And secondly, you’ll probably be interested in what the Kentucky Board of Medical Licensure had to say following my testimony. The board’s “prepared statement” is only about 4 1/2 minutes, but there’s a lot to unpack here…
These two presentations before the Interim Joint Committee on Health Services represent two distinctly different approaches to a problem — one by caregivers, the other by regulators. Decide for yourself which approach is most vital in this moment of crisis.
Reading a prepared statement, President Thornbury said, “The board must make decisions based on the realities of the Commonwealth, not idealized scenarios.”
Well, the reality is that our young people are dying.
Kentucky’s buprenorphine regulation is outdated, harmful, and unsalvageable. It’s not necessary. And it forces physicians to practice beneath the standard of care. This regulation needs to be repealed, not processed, analyzed, and amended over a period of years. People who could be saved are dying now because of this regulation.
And, by the way, choosing life over death happens to be an “idealized scenario” I’m OK with.
Repealing 201 KAR 9:270 is choosing life.
Let’s make that the reality of our Commonwealth.
In summary…
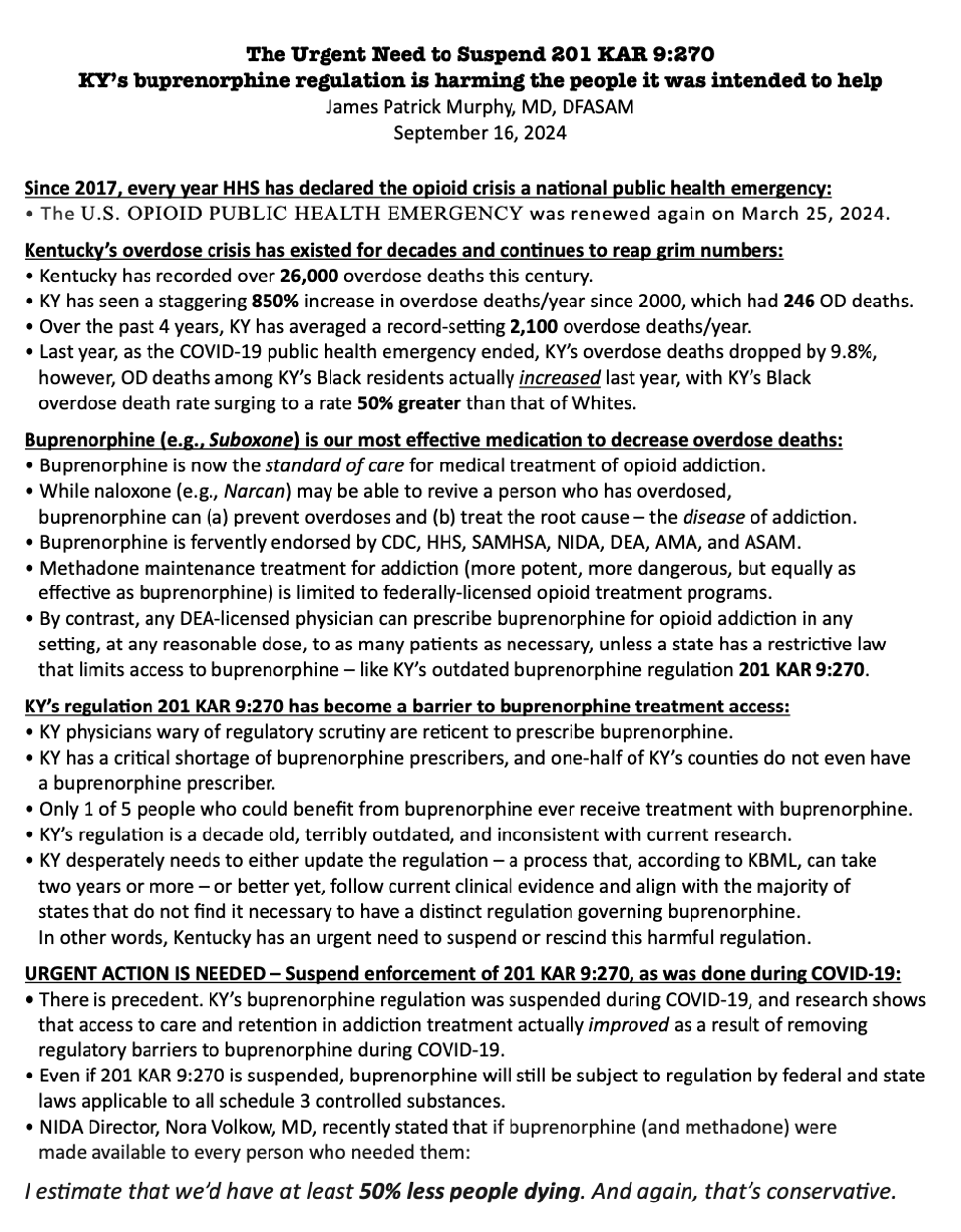
Kentucky is mired in the throes of a deadly public health emergency, an opioid overdose crisis that has taken the lives of over 26,000 of our neighbors, friends, family members, and loved ones since the year 2000. Buprenorphine, a DEA schedule III controlled medication, has emerged as an essential standard of care for the treatment of opioid use disorder. However since 2015, Kentucky physicians’ efforts to effectively care for patients with addiction have been hampered by a regulation, 201 KAR 9:270, that impedes access to life-saving treatment for Kentuckians most at risk of dying from an overdose. 201 KAR 9:270 forces physicians to practice below the standard of care. This is harmful to the citizens of Kentucky and worsens our state’s opioid crisis. As scholars of addiction treatment policy have explained, no evidence supports the requirements in 201 KAR 9:270, which by preventing access to buprenorphine, allows preventable deaths to occur. Kentuckians are needlessly dying because of this regulation.
On September 20, 2024, NIDA Director, Dr. Nora Volkow, gave the keynote address at UofL’s Research!Louisville awards ceremony. Here’s some of what our nation’s top addiction researcher had to say…
The opioid crisis started more than two decades ago, and we have not solved it.
It has caused more people dying than COVID itself.
The people that have died from the opioid crisis, all of them could have been prevented. Every single one of them could have been prevented.
We know how to prevent an overdose.
Overdoses are happening throughout all of the ages, throughout the whole life span.
The rise in overdose crisis…they went up to 117,000 in one year, those numbers were driven predominantly by fentanyl.
We are seeing the decreases in fentanyl overdoses…the latest numbers are twelve percent (decrease).
Pain medications started the overdose crisis. It basically stabilized and it’s going down.
Similarly, heroin basically is accounting for a very very limited amount of overdoses. And this reflects the fact that the drug dealers actually don’t see any benefit for them, incentive for them, selling heroin. They sell fentanyl.
What has created the turn down of the curve (in overdoses)?
This is what’s likely to be accounting for it… In the field of opioid use disorder, which is different from actually any other field in the substance use disorders, we have extremely effective medications.
To start with, we have an incredible drug, naloxone. Naloxone is an opioid receptor antagonist.
When you give it (naloxone) to someone that overdoses, you reverse that overdose if they overdosed with an opioid…Whether it is fentanyl or heroin or an opioid medication, you need to give the naloxone, for it to be effective, rapidly and at the correct dose.
We are very lucky to have naloxone.
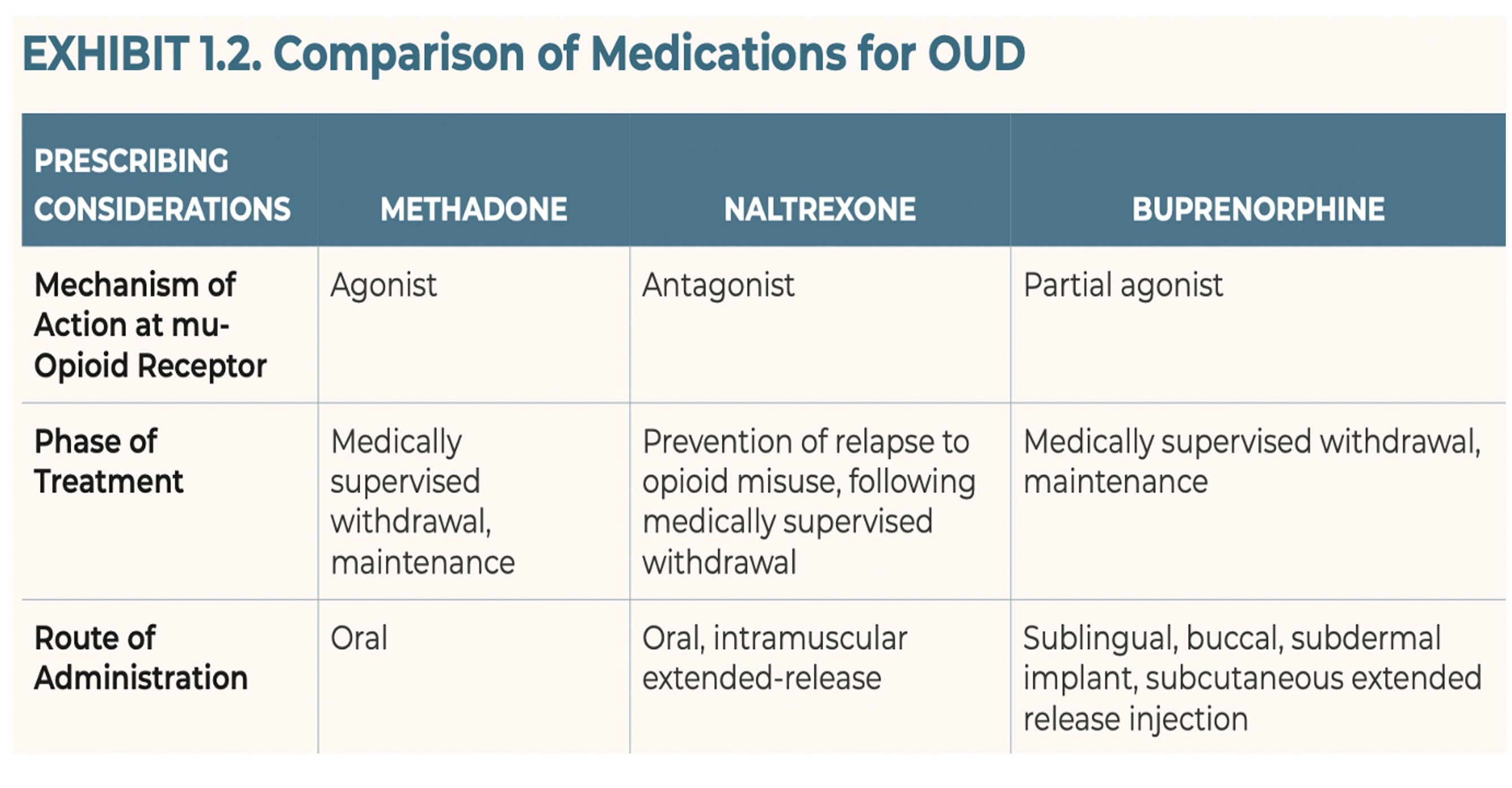
And then we have three different classes of medications, all targeting the opioid receptor system, but with different pharmacological effects, that are very effective in treating opioid use disorders.
Methadone…It has been in existence for, I think, sixty years.
Buprenorphine was approved at the beginning of the 2000s.
And then we have naltrexone, that was approved for opioid use disorder more recently.
Methadone – full agonist at the opioid receptor.
Buprenorphine – partial agonist.
These medications (methadone and buprenorphine) are effective in reducing drug taking, in reducing craving, in reducing withdrawal.
Except for naltrexone. Naltrexone does not, per se, reduce withdrawal, it reduces craving, and it improves mood.
They are very effective in preventing overdose.
So the challenge is, you say, if you have these medications that are being so effective, why are we having so many people dying of overdoses? And the answer is because we do have the medications, but they are not being given to those that need them.
Why are they not being used?
There are multiple issues.
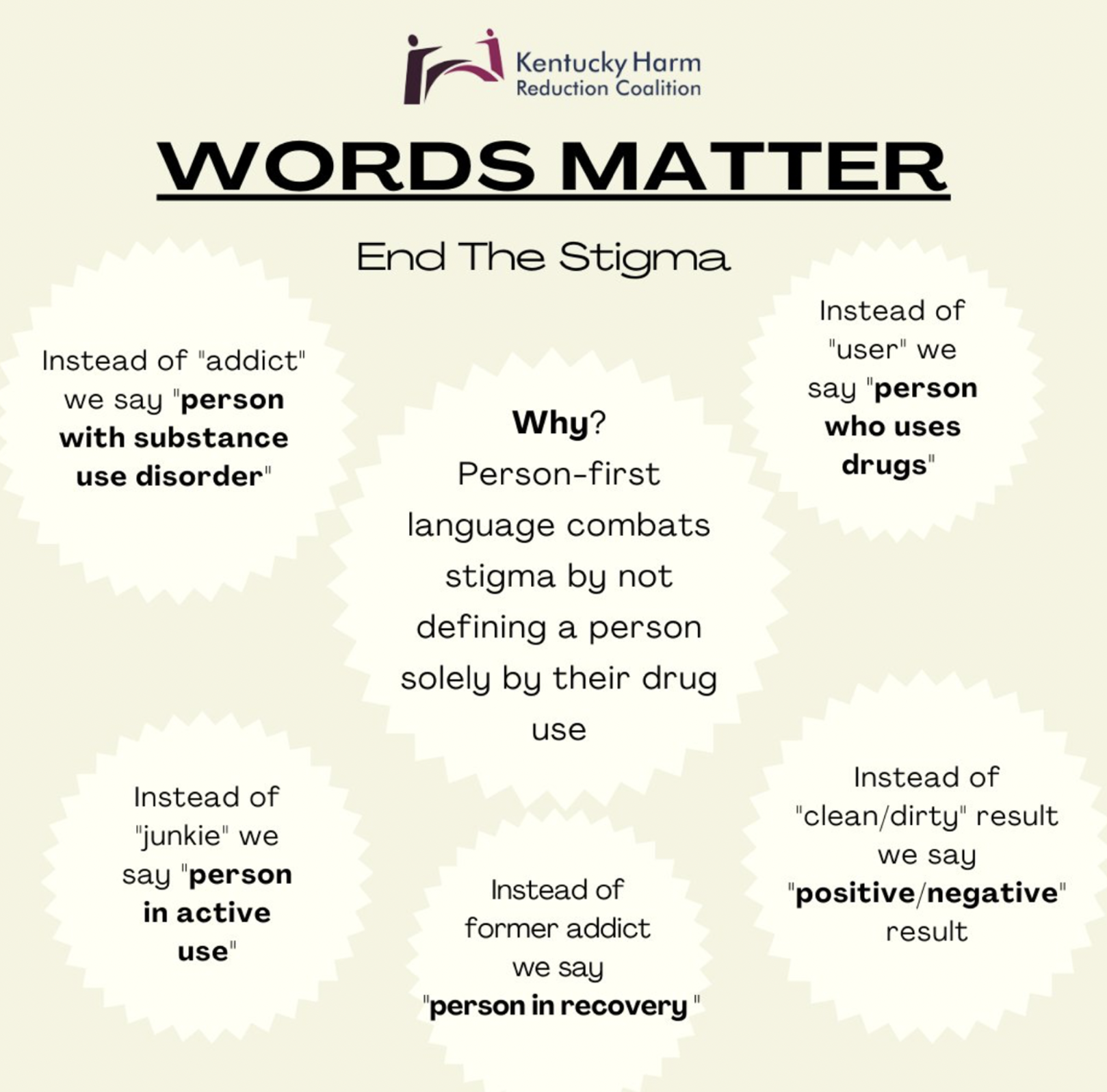
A key one is the stigma and discrimination against addiction.
The healthcare system providers don’t want to treat people with a substance use disorder.
We have generated a specialized system for the treating of substance use disorders that is independent of the healthcare system. Which is a totally lost opportunity.
Across the continuum, how can we improve access to these medications for people that need them?
There’s no evidence, to my knowledge, that any of the harm reduction practices exacerbate or increase the rate of overdose. I don’t know of any evidence. On the other hand, there’s ample evidence to show that harm reduction practices significantly reduces mortality.
There was so much expectation that the removal of the (DEA) waiver would increase the number of practitioners prescribing buprenorphine, but it hasn’t happened. What the research has shown is that the number of prescribers giving buprenorphine has not increased very much…Restrictive practices don’t help…The issue to me, this is discrimination. There is discrimination also in the way that we set up the reimbursement of taking care of someone with a very complex and potentially fatal disease.
Thank you, Dr. Volkow. You knocked it out of the park!
And this statement by our NIDA Director bears repeating, because it is a call to action: “If you have these medication that are being so effective, why are we having so many people dying of overdoses? And the answer is because we do have the medications, but they are not being given to those that need them.“
On September 19, 2024, I did two things via the Kentucky Governor’s official website: (1) I requested a meeting, and (2) I sent him an email via https://governor.ky.gov/contact.
Hint: Anyone can do this.
Here’s my email to Governor Andy Beshear.
Dear Governor Beshear,
This could be the most important message you get today. I appreciate you for taking the time to read it. And first of all, let me thank you for your amazing support of patients, families, and caregivers struggling to battle the disease of addiction and its tragic effects on the lives of Kentuckians.
I was standing in that bright sun on the front row just to your right on Monday’s inspirational Recovery Monthevent. After attending, I am more certain than ever that KY in general, and you in particular, are truly dedicated to defeating KY’s opioid crisis — the most deadly public health emergency in our lifetime.
As I heard you speak, along with the distinguished people to your left and right, and later as I walked along that road between the Capitol and the Annex, meeting the numerous groups representing KY’s amazing response to the crisis, I really felt that united we were standing against this disease, and that we are making some progress.
And as a physician who follows scientific evidence, I’m happy I get to inform you that there is still something you can do. There’s something standing between you and your goal, but it’s fixable.
That’s good news, Governor!
I’m referring to KY’s buprenorphine regulation 201 KAR 9:270. It’s outdated and is harming the people it was intended to help. It gets in the way of KY physicians’ willingness and ability to prescribe this lifesaving medication. Something needs to be done about it. It needs to go.
I’m not a politician, not a lawyer, not a regulator. I’m a doctor. I speak for my patients, my colleagues, and the thousands of Kentuckians who could be saved by universal access to buprenorphine.
But you don’t have to take my word for it. I am certain you know of NIDA Director, Dr. Nora Volkow. I’m equally certain you trust her. Well, she has recently stated that the overdose rate in our country could be cut in half if everyone who needs buprenorphine could find access to it. Dr. Volkow has the research data to back up that claim. And, by the way, I’m meeting her at UofL tomorrow at the Louisville!Research event. Yes, I’m having a really good week!
Governor Beshear, I know in your heart and in your mind you want to do everything you can to save lives. I know it is personal to you. And I promise, if you can find some way to get rid of this outdated, unnecessary, and harmful regulation, my colleagues at KYSAM and ASAM and I will do everything we can to make certain your action in this matter will result in tremendous success — and by “success” I mean, thousands of lives saved.
Just ask yourself, is there anything else you can think of that is (a) so supported by science, (b) so supported by experts, and (c) so simple to do? You and your administration have already done so much. And you’ve had some success for sure. That’s commendable and something to celebrate. And how great would it be to stand up to the podium on the south lawn next year and be able to say that KY’s overdose deaths have been cut by 50% !
This is not just hopeful, this is do-able! Trust the science.
Governor Beshear, you work so hard, you put your heart and soul into this cause every day. You deserve to get a better return on your investment. KY needs to get a better return on your investment. And we can!
On Monday 9/16/2024, under a brilliant baking sun, from the south lawn of the state Capitol, Governor Andy Beshear proclaimed September to be Recovery Month in Kentucky. To his left and to his right sat about twelve sun-drenched dignitaries, most wearing business attire meant for air-conditioned offices. As I stood there in the front row, myself baking in the sun, I realized two things early on: (1) I had made the right decision to come, and (2) my game time decision to wear my UofL Med School polo shirt instead of a coat and tie was the right move (Can you find me in the pic below?).
Screenshot
I’d never heard Governor Beshear speak in person, and I found him to be as charming, personable, likable, and relatable as he always appears to be on TV. The governor said all the right things that needed to be said. He was inspirational as he recounted the work that had been done by Kentucky’s government over the past year battling the opioid crisis in our state. He touted KY’s 9.8% drop in overdose deaths from a year ago. He also said “There is a lot of work left to do.”
Eric Friedlander, Secretary of KY’s Cabinet for Health and Family Services also spoke and said he is thankful he is working for a Governor who “believes in science.”
And Lisa Lee, Commissioner for the Dept. for Medicaid, said that we’ve made progress, but she won’t be satisfied “until all barriers to treatment are gone.”
Others eloquently spoke, bills were ceremoniously signed, a few people with lived experience offered their compelling stories to the crowd, which dwindled a bit over time as onlookers gradually receded into the few shady spots farther away from the podium. All in all, the message was very positive. And as I stood in the front row to the right of the stage, facing Representative Kim Moser, the only other person besides me wearing red in Frankfort that day, I really wanted to believe the Governor when he said in closing, “I am convinced that we can defeat this epidemic.”
After the speeches, Representative Moser visited with me, offered me some of her views, gave me a little advice, and graciously invited me to come back to Frankfort in October to testify before her colleagues. She also introduced me to Secretary Friedlander, who I chatted with briefly. And before I left the podium area I got to speak with a true KY hero, Van Ingram, Executive Director for the Kentucky Office of Drug Control Policy.
These were all great connections to make. I had travelled to Frankfort thinking my main objective was to meet some of the people who I’ve been emailing regularly about the urgent need for a major overhaul of KY’s outdated and harmful regulation governing how physicians prescribe buprenorphine to treat addiction. I felt that my meet-and-greet mission had been accomplished. I could now report back to my organizations (i.e., KYSAM, ASAM, AMA, KYHRC) that our concerns about the buprenorphine regulation were probably a little closer to getting heard by the people who could bring about the needed change.
What happened next was unexpected.
I walked to the far end of the road between the Capitol and the Annex Building where dozens of addiction treatment, addiction recovery, and addiction support groups had set up tents, tables, and booths. I decided to visit every group represented there. I learned what they did, how they were funded, what role they played in the orchestra of helpers throughout our state. I met some amazing people, and I am definitely going to follow up with as many as I can. We truly have some fantastic advocates and caregivers in our state.
And maybe providence had a plan for me that day, because as I worked my way along that road from the far end to the beginning, near the humongous, beautiful, and famous floral clock on the Capitol grounds, the last group I visited was comprised of only two women. Out of respect for their privacy, I won’t go into specifics. But suffice it to say, these two amazing individuals were living fulfilling lives in recovery from opioid addiction, both were being treated with buprenorphine, and both told me that treatment with buprenorphine had literally saved each of their lives.
With this as my send off, I left the Capitol a little more sunburned but tremendously more inspired. It’s clear, there are a lot of wonderful people in our state doing fantastic things to help people with addiction make it to their promised land of recovery. And I’m more determined than ever to prove myself worthy of inclusion amongst the ranks of these dedicated and compassionate healers, by virtue of my doctoring, my advocacy, and my caring.
If you’ve read all the way down to this point in my article, then you are likely one of those wonderful people I mentioned in the paragraph above – because I know my writing is nowhere near as compelling as the cause. And you’re probably a person who wants to make a difference – maybe even save a life in the process. If so, then I have an ask of you…
Please help me get the message to our Governor that Kentucky’s outdated buprenorphine regulation needs to be gone. The science, the data, and the lived experience of thousands in recovery confirm that buprenorphine treatment for opioid addiction promotes recovery, prevents overdoses, and saves lives. I made some handouts that I gave to people at the Recovery Month event on the Capitol lawn. Below you will find screen shots of the handouts.
As I said to one nice young lady, who politely told me that because she was employed by the state there was no way she could advocate for changing a state regulation, “That’s all right. I’m just asking that you read it.”
“Why?” she asked.
“Because, once you read it, you can’t un-read it.”
So, now I humbly ask you to please read the information below. And if you want to help remove a significant barrier to people with addiction receiving the most effective treatment we have to prevent overdoses and promote recovery, then stoke your creativity, ingenuity, determination, and problem-solving skills and help me find a way to get this information to Governor Beshear.
As Secretary Friedlander said, our Governor believes science.
Dr. James Patrick Murphy is spearheading an opportunity for stakeholders to sign onto a letter to the Kentucky Board of Medical Licensure (KBML) urging it stop finalization of proposed changes to 201 KAR 9:270, a regulation governing the prescribing of buprenorphine for the treatment of opioid use disorder (OUD), and instead form a new workgroup charged with conducting a thorough review of the regulation and recommending revisions through a transparent process.
The KBML’s current proposed changes risk perpetuating severe harm during a rapidly evolving addiction and overdose crisis, are inconsistent with evidence-based practice, create new treatment barriers, and may even worsen the addiction and overdose crisis in Kentucky.
Please also note you will also be subject to the following disclaimer if you sign the letter:
“The views expressed herein are those of the individual signatories and do not necessarily represent the views of their institutions or organizations.”
Ask: The KBML needs to convene a new workgroup of diverse experts and stakeholders and extensively overhaul the current regulation.
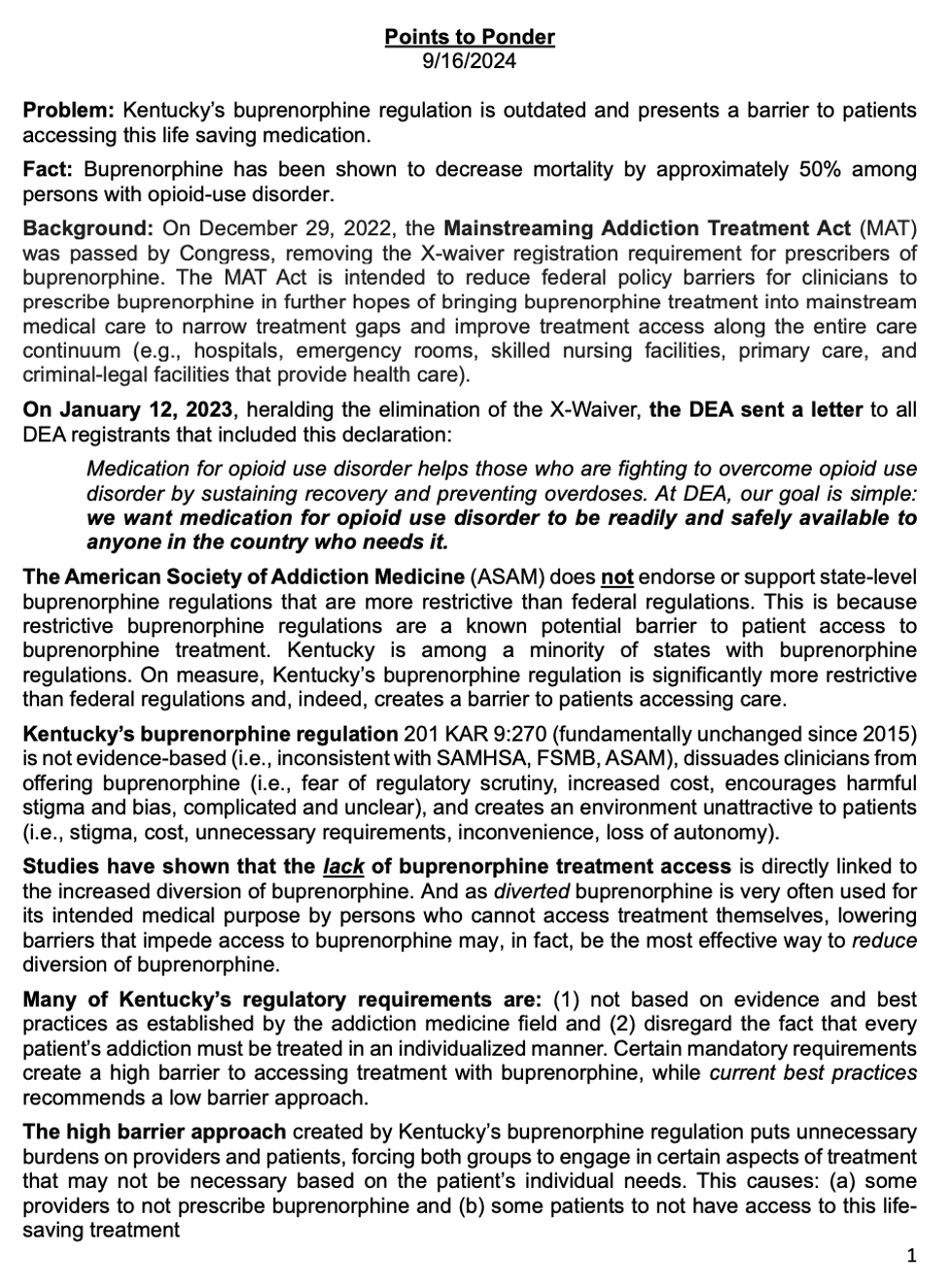
Fact: Buprenorphine has been shown to decrease mortality by approximately 50% among persons with opioid-use disorder.
Background: On December 29, 2022, the Mainstreaming Addiction Treatment Act (MAT) was passed by Congress, removing the X-waiver registration requirement for prescribers of buprenorphine. The MAT Act is intended to reduce federal policy barriers for clinicians to prescribe buprenorphine in further hopes of bringing buprenorphine treatment into mainstream medical care to narrow treatment gaps and improve treatment access along the entire care continuum (e.g., hospitals, emergency rooms, skilled nursing facilities, primary care, and criminal-legal facilities that provide health care).
On January 12, 2023, heralding the elimination of the X-Waiver, the DEA sent a letter to all DEA registrants (see DEA letter), that included this declaration:
Medication for opioid use disorder helps those who are fighting to overcome opioid use disorder by sustaining recovery and preventing overdoses. At DEA, our goal is simple: we want medication for opioid use disorder to be readily and safely available to anyone in the country who needs it.
The American Society of Addiction Medicine (ASAM) does notendorse or support state-level buprenorphine regulations that are more restrictive than federal regulations. This is because restrictive buprenorphine regulations are a known potential barrier to patient access to buprenorphine treatment. Kentucky is among a minority of states with buprenorphine regulations. On measure, Kentucky’s buprenorphine regulation is significantly more restrictive than federal regulations and, indeed, creates a barrier to patients accessing care.
Kentucky’s buprenorphine regulation201 KAR 9:270 (fundamentally unchanged since 2015) is not evidence-based (i.e., inconsistent with SAMHSA, FSMB, ASAM), dissuades clinicians from offering buprenorphine (i.e., fear of regulatory scrutiny, increased cost, encourages harmful stigma and bias, complicated and unclear), and creates an environment unattractive to patients (i.e., stigma, cost, unnecessary requirements, inconvenience, loss of autonomy).
Studies have shown thatthe lack of buprenorphine treatment access is directly linked to the increased diversion of buprenorphine. And as diverted buprenorphine is very often used for its intended medical purpose by persons who cannot access treatment themselves, lowering barriers that impede access to buprenorphine may, in fact, be the most effective way to reduce diversion of buprenorphine.
Many of Kentucky’s regulatory requirements are: (1) not based on evidence and best practices as established by the addiction medicine field and (2) disregard the fact that every patient’s addiction must be treated in an individualized manner (see Michelle Dr. Lofwall’s op-ed below). Certain mandatory requirements (see list below) create a high barrier to accessing treatment with buprenorphine, while current best practices recommends a low barrier approach (see SAMHSA Advisory on low barrier models of care).
The high barrier approach created by Kentucky’s buprenorphine regulation (see KYSAM letter) puts unnecessary burdens on providers and patients, forcing both groups to engage in certain aspects of treatment that may not be necessary based on the patient’s individual needs. This causes: (a) some providers to not prescribe buprenorphine and (b) some patients to not have access to this life-saving treatment
Required visits and frequency of visits (i.e., should be determined by an individual clinician based upon clinical judgment and the individual needs of the patient).
Requirements for in-office initiation vs. home initiation of treatment with buprenorphine.
Non-evidence-based limitations and restrictions on buprenorphine monoproduct vs. buprenorphine/naloxone combination.
Prescriber qualifications to prescribe buprenorphine products to treat OUD (i.e., educational requirements, X-waiver).
The appropriateness of co-prescribing buprenorphine with other medications such as benzodiazepines and gabapentin.
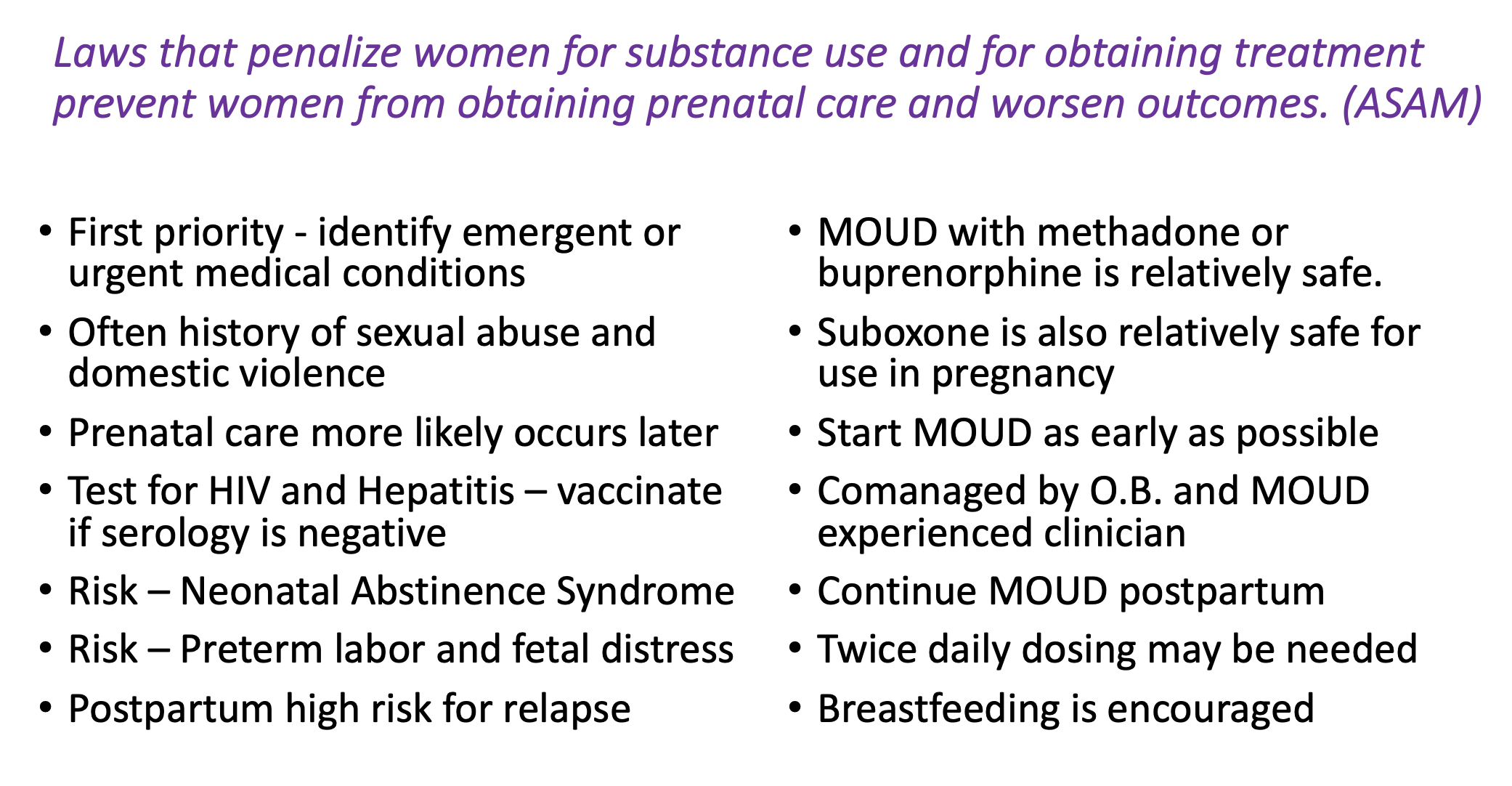
Appropriate treatment of pregnant patients, e.g., requirement for an independent consultation prior to initiating treatment.
Quantity limits on buprenorphine (i.e., dose limits).
Requirements for counseling or other behavioral modification services.
Mandatory urine drug testing (e.g., frequency, number and specific drugs tested).
Mandatory lab testing (e.g., pregnancy, HIV, Hep C, etc.)
Restrictions on off-label use of buprenorphine for pain management.
Guarantees against drug interactions.
Mandatory use of subjective clinical tools (e.g., a COWS scale).
Requiring patients to report the lost or stolen medications to police or other law enforcement agencies, which is punitive and unnecessary, as this could prevent patients from returning to treatment if their medication is lost, stolen, or diverted. Such requirements can put patients’ lives at risk.
Summary: Because each patient is unique, and because scientific knowledge and clinical best practices change over time, Kentucky’s buprenorphine regulation must allow for care that is informed by:
(1) the needs of the individual patient,
(2) the changing body of scientific and clinical knowledge, and
(3) the clinical judgment of the physician.
Kentucky’s current buprenorphine regulation does not achieve this goal.
For the past three years,
Kentucky’s overdose death rate
has remained at or near a record high.
Kentucky’s current buprenorphine regulation is more harmful than helpful.
Change is needed.
Now.
Here is the petition you will be signing…
Dear President Thornbury:
As deeply concerned citizens of the Commonwealth of Kentucky, we write to urge the Kentucky Board of Medical Licensure (KBML) to (1) stop its current process of finalizing proposed changes to 201 KAR 9:270, a regulation governing the prescribing of buprenorphine for the treatment of opioid use disorder (OUD), and (2) form a new workgroup – charged with conducting a thorough review of the regulation and recommending revisions through a transparent and open process. While we are incredibly grateful for KBML’s recognition of the urgent need to update 201 KAR 9:270, KBML’s currently proposed changes risk perpetuating severe harm during a rapidly evolving addiction and overdose crisis.
On or about June 4, 2024, KBML informed several stakeholders of an updated draft of 201 KAR 9:270, aimed “to bring the regulation into conformity with current acceptable and prevailing professional standards.” However, the proposed changes will not achieve KBML’s stated goal. They are inconsistent with current evidence-based practice, create new treatment barriers, and may even worsen Kentucky’s addiction and overdose crisis.
Buprenorphine is a highly effective treatment for OUD, which reduces illicit opioid use, reduces pharmaceutical opioid misuse, decreases risk for injection-related infectious diseases, and decreases risk for fatal and nonfatal overdoses. OUD treatment with buprenorphine is also associated with reduced general health care expenditures and utilization, such as fewer inpatient hospital admissions and emergency department visits. Despite buprenorphine’s effectiveness in significantly cutting opioid-related mortality, less than 20% of people with OUD receive medications for their disorder, partly due to regulatory barriers like those in Kentucky’s 201 KAR 9:270.
In fact, if KBML does not reopen its rule process and address 201 KAR 9:270’s requirements that interfere with a physician’s ability to exercise proper clinical judgment, then the consequences for the Commonwealth will be severe. Continuing to restrict appropriate access to treatment for OUD with buprenorphine increases the risk of non-fatal and fatal overdoses, overall health care costs, and fear among physicians and patients alike. We only further strain Kentucky’s safety net hospitals and emergency departments whenever rules dissuade physicians from appropriately treating OUD with buprenorphine. Indeed, failure to reopen KBML’s rule process means gambling with the lives of every Kentuckian. That is unacceptable – but fixable – if KBML reopens the process and halts pending rules that can cause unnecessary suffering and death.
In 2015, KBML promulgated its first version of 201 KAR 9:270. That year, there were 1,219 overdose deaths in Kentucky. KBML last updated the regulation in 2021, a year in which Kentucky experienced 2,250 overdose deaths – the highest annual number on record in the Commonwealth. In 2022, there were 2,135 overdose deaths, and in 2023 the total was 1,984. In sum, since the initial 2015 regulation, overdose deaths in Kentucky are more than 60% higher as of 2023. Revising the regulation now – without ensuring transparency, avoiding conflicts of interest, incorporating high- quality evidence, clearly articulating recommendations, and fully engaging stakeholder review – will only perpetuate the regulation’s unintended barriers to lifesaving care.
In addition, it is important to note that both a recent publication by the Substance Abuse and Mental Health Services Administration and a recent position statement of the Federation of State Medical Boards emphasize the need to reduce barriers to appropriate access to buprenorphine for the treatment of OUD. Both also highlight that policies can often hamper life-saving treatment with buprenorphine.
Furthermore, medical ethics require physicians to respect the law while recognizing their ethical responsibility to seek changes in those requirements which are contrary to the best interests of patients.
For all these reasons, we humbly urge KBML to stop the process of finalizing the currently proposed changes to 201 KAR 9:270 and to form a new workgroup. This new workgroup should include addiction medicine specialists, pain specialists, psychiatrists, primary care physicians, pharmacists, and patient advocates who share a common goal of recommending regulatory changes that will ensure competent, patient-centered addiction care, rooted in scientific evidence, clinical experience, nationally recognized guidelines, and expert consensus, as well as compassion, respect, and responsiveness to individual patient preferences, needs, and values.
Thank you in advance for considering this important request. We strongly support KBML’s mission to protect the public and promote the public welfare of the citizens of the Commonwealth, and we stand with you in that endeavor. If you have any questions, or wish to discuss this request further, please do not hesitate to contact Dr. James Patrick Murphy at james.murphy.2@louisville.edu.
Note: The views expressed herein are those of the individual signatories and do not necessarily represent the views of their institutions or organizations.
Sincerely,
Note: On 8/1/2024, the petition was hand-delivered to the KBML with 450 signatories. We have over 550 signatories now, and the list is growing. You can still sign on and join health care advocates like:
Brian Hurley, M.D. President, American Society of Addiction Medicine
Stephen M. Taylor, MD President-Elect, American Society of Addiction Medicine
Kelly J. Clark, MD, MBA, DLFAPA, DFASAM Past President, American Society of Addiction Medicine and Past President of KYSAM
Colleen Ryan MD, FASAM President-Elect, KYSAM
James Patrick Murphy MD, DFASAM Immediate Past President, Kentucky Society of Addiction Medicine (KYSAM)
And here’s the resolution that the Greater Louisville Medical Society will be preventing to the Kentucky Medical Association at KMA’s annual meeting August 23, 2024:
WHEREAS, according to the 2023 Kentucky Drug Overdose Fatality Report, 1,984 Kentuckians lost their lives last year to a drug overdose, which is more than a 50% increase from 2019; and WHEREAS, recent CDC data lists Kentucky as having the seventh highest overdose death rate in the country; and WHEREAS, recent CDC data indicates approximately 70% of overdose deaths are caused by opioids; and WHEREAS, buprenorphine treatment has been associated with more than a 60% reduction in the risk of opioid-involved overdose death; andWHEREAS, new research out of Kentucky, recently published in the Journal of Addiction Medicine, suggests that higher doses of buprenorphine are associated with reduced opioid-involved overdose deaths and death from other causes; and WHEREAS,201 KAR 9:270 is a recognized barrier to patients accessing treatment with buprenorphine; and WHEREAS, American Society of Addiction Medicine (ASAM) policy states it is vital that unnecessary and over-burdensome barriers to buprenorphine treatment be avoided so patients can have timely access to care; and WHEREAS, ASAM policyfurther recommends any state regulation regarding buprenorphine be evidence-based so as not to dissuade clinicians from offering buprenorphine treatment, nor create environments unattractive to patients because of unnecessary and unhelpful regulatory burdens; and WHEREAS, 201 KAR 9:270 is seriously outdated and long overdue for a review and update; and WHEREAS, on or about June 4, 2024, KBML informed stakeholders of an updated draft of proposed changes to 201 KAR 9:270; and WHEREAS, the Kentucky Society of Addiction Medicine and other field experts, have reviewed the KBML’s proposed changes to 201 KAR 9:270 and have concluded that the proposed changes will create environmentsunattractive to patients because of unnecessary and unhelpful regulatory burdens and will not bring the regulation in accord with evidence-based practicebut will instead create new treatment barriers and may even worsen Kentucky’s overdose crisis; now therefore be it RESOLVED, that KMA call upon the Kentucky Board of Medical Licensure (KBML) to stop KBML’s process of finalizing proposed changes to 201 KAR 9:270 and promptly convene a diverse workgroup, comprised of experts in the field, tasked with recommending regulatory changes that will ensure competent, evidence-based, and patient-centered treatment of opioid use disorder with buprenorphine.
Science-Based Addiction Treatment Must Drive U.S.Policy
Dr. Michelle Lofwall
June 17, 2024
When you’re sick, you go to the doctor.
When you have a life-threatening disease, you get medical treatments to save your life.
When you have opioid use disorder (OUD), you can hit a brick wall, because America’s healthcare systems cannot always deliver the care you need. This is true for several reasons, including stigma, a lack of understanding that addiction is a treatable, chronic medical disease, and an array of restrictive policies and practices, including federal legal barriers that prohibit your state from providing access to one (i.e., methadone) of three OUD medications through prescriptions dispensed from your nearby pharmacy.
In the era of high-potency synthetic opioids, like fentanyl, expanding access to life-saving medications for OUD, particularly methadone and buprenorphine, is critical. Both medications are associated with reduced mortality in people with OUD. They help doctors treat addiction and save lives at a time when opioid-involved overdose deaths are near historic highs. While the latest statistics show the first nationwide drop in overdose deaths in 5 years and an even bigger drop in Kentucky, many states are actually recording significant increases, and Black and Indigenous Americans are still disproportionately more likely to die from an opioid overdose. Illicitly manufactured synthetic opioids can be much more powerful—and deadlier—than heroin and are flooding our communities. Since opioid withdrawal isso excruciating, people with untreated OUD often seek out illicit opioids to prevent pain –– both physical and emotional –– even when they want to stop using them. In contrast, methadone and buprenorphine are proven to help people with OUD manage their disease and be part of the recovery process. New research out of Kentucky, recently published in the Journal of Addiction Medicine, suggests that higher doses of buprenorphine are associated with reduced opioid-involved overdose deaths and death from other causes. Relatedly, methadone may be needed for patients who don’t respond well to buprenorphine. Yet, physicians, even those who are experts in treating addiction, are not always trusted to make appropriate clinical decisions when it comes to these medications.
Unfortunately, despite the recent elimination of a registration requirement for prescribing buprenorphine for OUD, buprenorphine continues to be hindered by burdensome policies, such as non-evidence-based state regulations and unnecessary prior authorization requirements by insurers, even on injectable formulations that cannot be diverted by patients. All these hurdles impede timely access to buprenorphine for OUD and fuel our overdose crisis. Similarly, methadone’s potential is limited by a 50-year-old federal law that is preventing regulators from even trying to increase access to it through prescriptions dispensed from community pharmacies – an approach that has been used successfully in other countries for decades. Consequently, patients who need methadone for OUD must visit one of approximately 2,100 opioid treatment programs (OTPs) in the United States to get their medicine, and for those who can access an OTP, it can still be difficult for some to stay in methadone treatment and maintain their recovery. While OTPs play an important role in the addiction treatment continuum, it’s past time for Congress to pass federal legislation that would empower federal and state regulators to determine how best to access methadone prescribed by addiction specialist physicians for OUD through local pharmacies, which overwhelmingly outnumber OTPs.
Tragically, concerns around methadone and buprenorphine diversion tend to slow necessary reforms. While diversion concerns must be considered and appropriately addressed, they should represent only one aspect of our national conversation when it comes to life-saving medications for OUD, not dominate it. Outdated laws, regulations, and policies governing both buprenorphine and methadone for OUD are failing to meet the moment—and worse, are exacerbating the deadliest overdose crisis in American history.
Dr. Michelle Lofwall is board-certified in psychiatry and addiction medicine. She is a professor of behavioral science and psychiatry and the Bell Alcohol and Addictions Chair at the University of Kentucky College of Medicine. The views expressed herein are those of Dr. Lofwall and do not necessarily represent the views of the University of Kentucky.
Signatories to the petition delivered on August 1, 2024 include:
Melissa Dye, Patient Advocate,
Grieving mother to my 23 year old Marine son who lost his life to an overdose,
PMHNP-BC
Debbie Henderson-Thomas
Past board member of Kentucky Harm Reduction Coalition
Grieving mother
Brian Hurley, M.D.
President, American Society of Addiction Medicine
Kelly J. Clark, MD, MBA, DLFAPA, DFASAM
President, Addiction Crisis Solutions, Louisville, KY
Past President, American Society of Addiction Medicine
Past President, KYSAM
Russ Farmer, Sr. Associate Dean,
University of Louisville School of Medicine
Maria Braman
Appalachian Regional Healthcare
Rep. Kimberly Moser
State Representative, 64th District; Chair, House Health Services
Jason M. Nemes
Commonwealth Counsel Group
James Patrick Murphy MD, DFASAM
Immediate Past President, Kentucky Society of Addiction Medicine (KYSAM)
Colleen Ryan MD, FASAM
President-elect, KYSAM
Michelle Lofwall MD, DFASAM, DFAPA
Professor of Behavioral Science and Psychiatry,
University of Kentucky
Dr. Kimberly Alumbaugh, FACOG
Past President Greater Louisville Medical Society
James B. Tabler MD
Retired Physician
Paul E. Brown MD
Gastroenterology Health Partners
Michael C. Cronen DO
The Pain Institute
Oliver Benes MD, FASAM, FAAFP
Saint Elizabeth Physicians Journey Recovery Center
Anthony E. Martin MD
Physician
Mitchell Simons MD
Self-employed Physician
Katlynn White
Saint Elizabeth Physicians Journey Recovery Center
Jeffrey Alan Craven LMHC, LPCC, CADAC IV
Saint Elizabeth Physicians Journey Recovery Center
Stacey Gripshover PMHNP-BC, PMH-C
Saint Elizabeth Physicians Journey Recovery Center
Katrina Nickels MD, FASAM
Secretary, KYSAM
Assistant Professor, University of Kentucky College of Medicine,
Dept. of Internal Medicine
Logan Nellis
Saint Elizabeth Physicians Journey Recovery Center
Anna-Maria South MD
Physician
Devin Oller, MD, FASAM
Assistant Professor of Medicine,
University of Kentucky College of Medicine
Raven R. Piercey Ph.D.
Lexington, KY
Danielle Lenz PMHNP-BC
Melody Altschuler, Ph.D.
Eloise Fourie DO
Assistant Professor, University of Kentucky
Haley Busch, PharmD, BCPS
Opioid Stewardship Program Coordinator, CHI Saint Joseph Health
Stephanie Abel PharmD, BCPS
Opioid Stewardship Program Coordinator, University of Kentucky HealthCare
Brandon Kasberg, PharmD
University of Kentucky School of Pharmacy
Adjunct Professor, University of Kentucky Healthcare Pain Management and Palliative Care
Clinical Pharmacist
Karlee Daniels, APRN
Saint Elizabeth Physicians Journey Recovery Center
Monica F Roberts, PharmD
University of Kentucky Substance Use Priority Research Area
Alan Hall
Physician
Michelle Carlo
University of Kentucky
Sarah Edgerly, PharmD
University of Kentucky Pain Management and Palliative Care Pharmacy Specialist
Andrew Dues
St. Elizabeth Physicians Journeys Recovery Center
Danielle Anderson, MD
Addiction Medicine Specialist, Assistant Professor,
University of Kentucky College of Medicine
Brent Dinan
St. Elizabeth Physicians
Marianne Carter
University of Kentucky
Michael B. Flynn
Retired Surgical Oncologist
Zebulon South
Musician
Michael Thornton
Lloyd Trommler, MD
Internal Medicine
Sami El-Dalati
Assistant Professor of Infectious Diseases, Department of Internal Medicine,
University of Kentucky
Ryan Luse
HDD Worker
Jessica McFarlin
Division Chief Palliative and Supportive Care,
University of Kentucky
Emily Smith
Alteri Behavioral Health
Andi Stephenson, MSW, CSW
Mental Health Therapist
Laura Fanucchi, MD, MPH, FASAM
Physician, Associate Professor, University of Kentucky
James Troy, MD
Michael Aines, APRN
Sharon L. Walsh, Ph.D.
University of Kentucky
Jered Waggoner, PA-C
University of Kentucky HealthCare, Dept. of Cardiothoracic Surgery
Emily Lile Chrysler, LCSW
Palliative Care
Hannah K. Knudsen, Ph.D.
Professor, Department of Behavioral Science, University of Kentucky
Mattie Baker
Patrick Grace, MD
Assistant Professor, University of Kentucky Department of Emergency Medicine
Shanna Babalonis, Ph.D.
University of Kentucky
Mark R. Behr, MD
Anesthesiology Associates
Cheryl A. McClain, MD
Brightview Addiction Centers
Julie Schroeder MD
The Healing Place
ReMind Health Group
Ankit Arora
Assistant Professor, Addiction Medicine, University of Kentucky
Mary Helen Davis MD
Integrative Psychiatry
Sandy Tiu Berger
Hospital Pharmacist
Lisa McAdams
Traditions at Camargo
Brandon Ho
University of Kentucky, MD
Discover Recovery, LLC
Madilyn Harris
University of Kentucky HealthCare
Cameron Murphy, MFA
Lee Gibson
Jennifer Jones
Fort Thomas, Kentucky
Adele Murphy
Greater Louisville Medical Society Alliance
Angela M McCurdy, PTA
The Springs of Oldham Reserve
Kara Kennedy, DO
Associate Professor, Department of Neurology, University of Kentucky
Lakshmi Naidu, MD
College of Medicine, University of Kentucky
Terry Lancaster
HM Solution Manager
Courtney Perry, DO
Assistant Professor, University of Kentucky
Debi McDonald
Healing The Children Kentucky
Katherine Crabtree MD MPH
Bluegrass Community Health Center
Jaryd Zummer, MD
University of Kentucky HealthCare
Keisa Fallin-Bennett, MD, MPH
Associate Professor of Family Medicine
Glenn M. Lipton, MD
Board-Certified in Addiction Medicine, Pain Management, and Anesthesiology
Nicholas D Annichiarico, DO
Assistant Professor, Physical Medicine & Rehabilitation
Medical Director, Inpatient Rehabilitation Services, University of Kentucky
Sara S. Salles, DO
University of Kentucky
William Harris, PharmD
University of Kentucky Health Care
Mahmoud Amr
Hospitalist, University of Kentucky
Barbara V. Parilla, MD, FACOG, FASAM
Professor of Obstetrics and Gynecology,
University of Kentucky College of Medicine, Lexington
Mary Rutherford, MD
Independent Physician, Addiction Specialist
Vijay Aluru
University of Kentucky
Katherine Culbertson, APRN
James D. Hawthorne MD
Associate Professor, University of Kentucky, Addiction Medicine Specialist
Benjamin Meadows
Alteri Behavioral Health
Lexi Dickerson
St. Elizabeth Journey Recovery Center
Katherine Twist MD
University of Kentucky
Tatum Zeller
St. Elizabeth Physicians Journeys Recover Center
Kathleen M. Yang MD
Addiction Medicine Specialist, St. Elizabeth Physicians Journeys Recover Center
McKenzie Clarke, LCSW
Bluegrass Care Navigators
Nicole Breazeale
Associate Professor of Community Development, University of Kentucky
Meagan Schaeffner
Assistant Professor of Medicine, University of Kentucky
Angela Beale Martin, MD
Obstetrics-Gynecology
Richard Cales, MD, FASAM
Chief Medical Officer, NuLease Medical Solutions LLC
Kayla M. Strother, MSN, AGPCNP-C
Addiction Consult and Education Service,
University of Kentucky HealthCare
KANPNM, KYSAM, ASAM
Carissa McCarthy
St. Elizabeth Physicians Journeys Recover Center-Addiction Medicine
Deana Andrews, MSN, APRN, FNP-C, CARN-AP
Addiction, Counseling, Education Services, University of Kentucky
Celia Castellanos
Internal Medicine, University of Kentucky
John Romond, MD
Associate Professor of Internal Medicine
Melissa. L. Zook, MD, FASAM, FAAFP, HIVS
London Women’s Care, Family Physician, certified in Addiction Medicine, HIV specialist
Alicia Atkerson, RMA
St. Elizabeth Physicians, Journey Recovery Center
Danielle Dicken
University of Kentucky HealthCare
Emily C Henderson
Pharmacist
Daniel T. Weaver, MD, FACP, FASAM
Associate Professor of Medicine, University of Kentucky
Patricia Santos
Division of Hospital Medicine, University of Kentucky
Steve T. Vogelsang MD, FASAM, ABPM, FAAFP
Dr. John J. Wernert
Norton Behavioral Medicine
Daniel Wolens
Clinician
James D Sams, MCSP
Sean F Martindale, MSN, APRN, FNP-C
Robley Rex VA Medical Center
Susan Stewart, RN
Reynold Andika
University of Kentucky Hospital
Jesse Caylor
Citizen of Kentucky
Dr. Margaret McGladrey
Assistant Professor, University of Kentucky College of Public Health
Rachele Yadon, MD
Kentucky Licensed Psychiatrist
Amber Silberman, APRN
University of Kentucky Palliative Care
Christopher Stewart, MD
Addiction Psychiatrist, Louisville KY
Amy Ward
LCSW, LCADC
Cooper Howard, CSW
Norma J Davidson
University of Kentucky
Michael Cherry, MD
University of Kentucky
Amy Preston LCSW
University of Kentucky Healthcare, SMART Clinic, LCSW
Kate Wimberly, MD
Assistant Professor, Internal Medicine and Pediatrics,
University of Kentucky
Pam Easterling
Saint Elizabeth HealthCare
Stephen Kyle Young, MD
Commonwealth Pain & Spine
Maureen Bensman
Licensed Professional Clinical Counselor
John Romond, MD
Associate Professor of Internal Medicine
Wm. Kelly Vincent, MD, DAAFP, DABPM, DASAM
Sam Yared, MD
Board Member, Greater Louisville Medical Society
Patricia Purcell MD MBA
Consulting
Erica Williams-Archie
Director of Operations, Kentucky Harm Reduction Coalition
Lewis Hargett, MD
President, Greater Louisville Medical Society
Stephanie L. Woods
Greater Louisville Medical Society
Frank Burns
Middletown Eye Care
Sarah Murray, DO
Assistant Professor, University of Kentucky
Vincent J. Blanch MD/PhD
KYSAM
Lewis Rowe
Kentucky Medical Association (KMA)
Lori Caloia MD, MPH, FAAFP
Mehak Pahwa, MD
University of Louisville
John D Rumisek MD, FACS
CT Surgeon (Retired)
Joshua Christensen, MD
NORTON HEALTHCARE
Cynthia Rauker Rigby, MD
retired OB/Gyn
Luke Roy MD
University of Kentucky
KEERTHI KEMPARAJURS
Lagrange Family Care Doctors
G. Randolph Schrodt, Jr. M.D.
Integrative Psychiatry
Margaret van Wyk
Norton Healthcare
Guy M. Lerner
Physician
Timothy J. Beacham, MD, FASA
Restorative Pain Institute
Barbara S Isaacs MD
Member of GLMS, KMA. AMA
Ali A. Farooqui, M.D.
Integrative Psychiatry, Integrative Psychiatry, PLLC; Clinical professor,
University of Louisville Department of Psychiatry
Audrey Summers, MD
Assistant Professor, University of Louisville
Department of Psychiatry and Behavioral Sciences
Kassidi Napier
MS4 at ULSOM
Brian L. Hawkins, M.D.
Community ENT & Allergy
Alyssa Ott
CRNA
John Herold MD
University of Louisville School of Medicine graduate
Carol Kulp-Shorten, MD
Clinical Professor of Medicine/Dermatology, UofL SOM
Heidi Moore
Sr. Director of Transitions of Care at UNIVERSITY OF KENTUCKY King’s Daughters
And ASAM Member, Sr. Director of Wellness and Recovery Program
Amy Pravin Shah, MD MBA MS
Howard Cohen MD
Board Certified in Pain Medicine,
Addiction, Psychiatry, Geriatric Psychiatry
and Psychosomatic Medicine
Luke Curtsinger
University of Louisville Class of 1985
J Thomas Murphy MD FRCPC FASAM
Professor Anesthesiology, perioperative, Pain and Critical Care Medicine
Julie Goldman
University of Louisville
Kayla Strother, MSN, APRN
University of Kentucky Healthcare, ASAM, KYSAM, KANPNM
Kevin J. Heine, MD
Baptist Health Gastroenterology
James B Eckman, Jr MD
Radiation Oncology – Baptist East Louisville
Sarah Acland
Retired
James Schuster.
University of Louisville School of Medicine graduate, 1985;
current Pennsylvania resident
Mary Lou Reichert, MD
KAFP
Ann E Giesel, MD
University of Louisville MD 1985
Jennifer Hollon MD
Nephrology Associates of Kentuckiana
Taryn Reynolds MSN APRN FNP-C
Rex Paul Lagerstrom, MD
Internal Medicine Consultant
John Pank, MD
ASA
Elizabeth F. Rouse, MD
University of Louisville, Family Medicine, Ret.
William T. Fannin, M.D. ABPM
East Kentucky Rehabilitation Centers
Stephanie Wilwayco, MD
U.S. Military Entrance Processing Station
Andrea Kristofy
Reverie Anesthesia, PLLC
Suresh Nair MD
Nair Internal medicine PLLC
Anthony Atala
U of L Medical School Class of 1985
Timothy Heine, MD
University of Louisville Physicians
Dr Jim Link
Practicing clinician
Jules Barefoot MD FASAM
Substance Abuse Consultants LLC
James B Eckman, Jr MD
Baptist Health Louisville
Sandra McGill
Retired
Brandon L Houk, MD, FASAM
Discover Recovery, LLC
John McGill
Humana
Rebecca Booth, M.D.
University of Louisville School of Medicine, Class of 1985
Steven Auden MD
Napdoc Inc.
Oliver C. James II, M.D.
Beale Recovery Centers
A Rodman Barber, MD
University of Louisville Medical School class of 1985
Rebecca Hamburger
University of Kentucky College of Medicine
Richard H Rhodes
Retired Pulmonary/Critical Care Medicine Community Hospital North
Jack Gerughty MD
University of Louisville School of Medicine, Class of 1985
Kimberly Miller
Advocacy Director for Kentuckiana Fibromyalgia Support Group
Thaddeus R Salmon M.D.
Internal Medicine & Pediatrics
Monalisa Tailor MD
Sarah E. Allen, MD
Professor of Medicine, University of New Mexico
Robert Liu
University of Louisville
Ed Monarch
McBrayer PLLC
Megan Tudor APRN
University of Kentucky HealthCare
Robert A. Zaring, MD, MMM, MSHI
Sarah Goedde MD
Resident Physician
Kellen Murphy
Medical Student, University of Louisville School of Medicine, Class of 2025
Harold Blevins M D
Retired
R. Corey Waller MS, MD
CMO, BrightView Health, Editor in Chief, The ASAM Criteria
Rachel Vickers-Smith
Assistant Professor of Epidemiology at the University of Kentucky
Joy Engblade, MD
University of Kentucky
Don Stacy II
M.D. dABR Radiation Oncologist ARH Cancer Center
J. Gregory Cooper MD
Family Medicine, Cynthiana
Lawrence Rueff, MD
Personal Physician PLLC
Norah B Wyatt
Chambers Trucking
Jeffrey M. Goldberg, MD
Fellow, American College of Obstetricians and Gynecologists
David L. Doering
MD, FACOG, FACS
Heidi Rodes Schweder, APRN
Alteri Behavioral Health
Anjum Bux MD
CEO Bux Pain Management
Denise Winland, MD
Charles Francke, MD
Ciara Lockstadt M.D.
University of Kentucky Department of Hospital Medicine
Eric Lydon M.D.
Independent Practicing Physician
Nathan Simmons
Grocery Category Manager Rainbow Blossom
J Thomas Murphy MD FRCPC
Professor, University of Kentucky, College of Medicine
La’Tonya R. Hocker, CSW
University of Kentucky Bluegrass Care Clinic
Alexander Bautista, MD, MBA, FASA
Professor, University of Louisville, Department of Anesthesiology and Perioperative Medicine
Lisa Hinkle
McBrayer PLLC
Yucui Chen, MD
Passport by Molina Healthcare
Kenneth Payne, FABAM, FACOG
Cassandra Almasri
University of Kentucky Medical School
Alicia Shirakbari, MD, ABPM, ABEM
Lydia Ratliff
Alteri Behavioral Health
Tanya Wozniak
MD, InnovaTel Telepsychiatry
Katherine Dedich
Omni Resource Services
S. E. McGee MD
Retired, Primary Care
Edward J. Dunn, MD
Associate Professor, University of Louisville School of Medicine and
Medical Director of Palliative Care, Jewish Hospital of Louisville
William Durkan
Baptist Health Hardin
Yucui Chen, MD
Passport by Molina Healthcare
Jesus Victor Tovar
Invictus4Core Behavioral Health and Addiction Medicine Owner and Provider
Dr. Sharon Walsh
University of Kentucky
JD Kolter, M.D.
Natalie G. Stephens, MD
Norton Healthcare
Kent L Davis MD, FAAFP, FASAM
Rose Uradu MD, ABPM, FASAM
Ultimate Treatment Center, Ashland KY
Sarah Rabe PA-C
St Elizabeth Physicians, Brighton Recovery Center
Jennifer Wood, MD
Assistant Professor, Department of Psychiatry,
University of Louisville School of Medicine
Lydia K. Tharp
McBrayer PLLC
Katy Harvey
McBrayer, PLLCR.
Todd Hockenbury, MD
Assistant Clinical Professor of Orthopedic Surgery,
University of Louisville School of Medicine
Bridget Scott
Paralegal
Robin Kindig
Internal Medicine and Pediatrics of Louisville
Christopher Anderson, MD
Commonwealth Pain and Spine
Karen C.Schwartz, DNP, WHNP-BC, GCSU
Cecil Peppiatt MD
Associate Professor of Medicine
Grant H. Breazeale, M.D.
Kentucky Physician
Rebecca Flora APRN
Saint Elizabeth Physicians
Perry Bohanon
St. Elizabeth physicians behavioral health
Clifford A Kaye MD
Associate Professor & Medical Director of Clinical Documentation Integrity,
University of Kentucky
Stephanie Merhar, MD MS
Neonatologist, Saint Elizabeth Healthcare Medical Staff
Allison Koetter, MD
Medical Director of Addictions, Seven Counties Services
Clayton M. Smith, MD, FACP
Associate Professor, University of Louisville
Jeremy Engel, MD
Member of the NKMS
Helen Rose McCoy Grimes, RN
Director of Nursing (Retired)
Susan Sawning
Associate Professor
Cheryl Baetzel RN, BSN
Debra Hardison, APRN-C
VIP Community Health LLC
Steven Passik
Pain and addiction trained Psychologist
Lynne Lanham
Omni Resource Services
Lori McAtee
Citizen
J. Michael Smitb
Private practice radiologist
Thomas J Schreiner MD, FACP
Carmen Pinto MD
Medical Director Communicare ACT team
Robert Jon Klickovich
Paradigm
Jude F Beyerle
Professional Engineer
Abel Sandman
stakeholder
Keith Carter MD
UL Health
Catherine Durkan, RN
Bill McAtee
Retired
Russell Patrick Ashford
CENTRA
John D Scott
Retired
Richard R. Morris, M.D.
ASA
Kelly Cooper, MD, MPH
Norton
Shawn A. Ryan, MD, MBA
BrightView Health
Darel Barnett MD
Baptist Health Pain Management Louisville
TImothy Ford
Associate Professor, Department Orthopaedics
University of Louisville
Emily Tarquin
Actors Theatre of Louisville
Dr. Teena Darnell
Bellarmine University
Denise Hasher Melancon
Personal Assistant
Sarah Ashford
United States Navy Petty Officer Second Class
Ricky Collis MD
Interventional Rehabilitation of Kentucky
Julie Marlow
Concerned citizen
James W. Foster, MD
MAT Physician, WestCare Tennessee
Dr. Douglas Gourlay
Retired, Pain and Chemical Dependency
Rachel PaulsonK.
J. Raeuchle
29th Street Communities
Lee J Kottak
Jeffrey B. Bringardner
President, Humana Health Plans of KY (retired)
Michael Staples
Healthcare Regulatory Compliance Expert and
Former State of Ohio Medical Board Investigator
Henry Lucas
Helena Grimes-Smith
Homemaker/farmer
Donald Davis
Co-Founder Kentucky Harm Reduction Coalition
Beth McBride
Retired
Rinkoo Aggarwal MD
Medical Director of Southern Indiana Rehab Hospital
Karen Doggett, APRN
Dr James P. Murphy – Murphy Pain Center
Jeremy Byard
The Arthur Street Hotel
Director of Harm Reduction
Phil Ward
Believer in saving lives
Amy Attaway
L. Chad Elder
Elder & Good, PLLC
Barbra Cave, PhD, APRN
University of Louisville
Karla McClain
MSN, PMHNP-BC, currently employed at the Lindner Center of Hope
Nicole Labor DO, BCFM, FASAM
Anna K. Dauer MD
Assistant Professor, University of Kentucky College of Medicine,
Department of Internal Medicine, Division of Palliative & Supportive Care
Kathryn Bundy
Patient Advocate
James Grenkoski
Brother of Dr. Mark Grenkoski
John L Robert’s, MD
Retired
John M Hall
Retired Machinist
Robert H Zax, MD
The Skin Group
Felicia Goodwin, MA
The Skin Group
Norma Goodwin
UPS Logistics
Karen Adams, LPN
The Skin Group
Stacey Swinford
The Skin Group
Kenneth Hamilton
R&L Carriers
Mark V Boswell MD
Retired Physician
Paul Blackburn, DO
Clinical Associate Professor, Department of Emergency Medicine,
University of Arizona College of Medicine-Phoenix, Phoenix, Arizona
Endy Cadet
Addiction Medicine Physician
Haley Pals, PharmD, BCPP
Psychiatric Addiction Pharmacist
James W Boone MD
Pediatric Cardiology
Claire Ellen Cowley, MD, FAAP
Retired Pediatrician , Gratis Professor, U of L Dept of Peds
Michael Kindred MD
Medical Director
C. Dean Furman, Jr.
Attorney
Eric Vessels, MD, DABA, DABPM
Sara Nelle Murphy
Kentucky Harm Reduction Coalition
Megan Ward
MD Student
Susan Riolo
Concerned Citizen
Edwin Brott, MD. MBA
Triangle Anesthesia, ARH Hazard
Mark G Smith MD
Orthopedic Surgeon
Concerned citizen
Retired (39years General Motors)
Rebecca Tamas, MD, DFAPA
Psychiatrist
Jacqueline Davis
Family APRN (retired)
Carol Hammerbeck, MD
Western State Hospital, Preceptor for Sullivan University School of PA Studies,
Medical Director Seasons Behavioral Health, Medical Director S&S Wellness Hub
Gerald W. Elliott, M.D.
Lexington Clinic Dermatology
Patricia Isaacs
Norton
Lynne Lanham
Omni Resource Services
Dr. Eric M DeYoung
Sophrosyne Integrative Rehabilitation
Tricia F Lister
Attorney
Ed Monarch
McBrayer PLLC
Shannon Huelsman, PA-C
Norton Children’s Orthopedics of Louisville
Richard H Rhodes, MD
CPCCM
Madonna Ringswald
Retired Physician, member AAPS, KOMA, KBML
Erica Sutton
Morehouse School of Medicine
O. Thomas Newcomb, III M.D.
St. Claire Health Care
John Hill, MD
University of Louisville Physicians
Standiford Helm MD
UCI Health Center for Pain and Wellness
David E. Sowa M.D.
University of Louisville School of Medicine,
1985 Class President
Elizabeth Salisbury-Afshar, MD,MPH
Addiction Medicine Physician
Teresa Parrott, MD
Retired Anesthesiologist
Ray C Kennedy MD
ER physician, Veterans Administration
Jeff Jones, MD
Chairman, Inspire Medical Louisville
Lagena Ison
Retired Clinical Nurse Specialist
Burr Brown
Brown & Millar
Alyssa M. Tremblay
Addiction Medicine Consult and Education Service, University of Kentucky
Jennifer Wood, MD
University of Louisville, Department of Psychiatry, School of Medicine
William W. Stoops
Courtney Eaves, DO
Psychiatrist at University of Louisville
Sanford M Silverman MD
Past President Florida Interventional Pain Physician
Past President Broward County Medical Association
Past Member American Society Addiction Medicine
Tracy L Ragland MD
OneFamilyMD PLLC
Andrea Baker
University of Kentucky HealthCare
Paige Walker, LCSW-S
University of Kentucky HealthCare
Angella Linder, Addiction Consult and Education Services,
University of Kentucky HealthCare
Stephen E. Fischer, MD
U of L School of Medicine Alumnus
James Jason Miller, MD
Robley Rex Veteran’s Administration Medical Center
David M. Stern, MD
Medical Director, Louisville Recovery Center
Valeryia Burshtein
Greater Louisville Medical Society
Eric Engelbrecht
University of Louisville School of Medicine
Matilyn Shanahan
University of Louisville School of Medicine
Noela Botaka
Medical Student at the University of Louisville School of Medicine
Shreeta Waldon
Kentucky Harm Reduction Coalition
Amy L Holthouser
University of Louisville School of Medicine
Kelly S. Ramsey, MD, MPH, MA, FACP, DFASAM,
Region 1 Director to the ASAM Board of Directors,
Immediate Past President of NYSAM
Board of Directors,
Addiction Medicine Physician and Addiction Medicine/Harm Reduction Consultant
Timothy J. Beacham, MD, FASA
Restorative Pain Institute; KYSIPP; GLMS; ASA; AMA
Joseph Greene
Louisville Hip and Knee Institute
Kenneth I. Freedman, MD, DFASAM
The Recovery Research Network
Laura Bishop, M.D., FACP, FAAP
Associate Professor, University of Louisville
Christina Jones, MD, FASAM, FISAM
Imperial Calcasieu HSA Behavioral Health
Johnathan Bilbro, M.D.
Assistant Professor, University of Louisville School of Medicine,
Department of Psychiatry and Behavioral Sciences
Kevin A. Sevarino MD, PhD
Medical Director, American Academy of Addiction Psychiatry
Relatively recently, I’ve participated in three presentations that I’d like to share: (1) Louisville Bar Association, (2) Louisville Forward Radio, and (3) the KY Harm Reduction Coalition
First is a discussion about the medical potential, as well as the risks, of marijuana.
Here’s four good references I used for the medical marijuana forum…
And second, I’d like to share a two-part discussion on “the opioid crisis” from Louisville Forward Radio…
Dr. Pat Murphy, pain and addiction specialist in a discussion with Mike Flynn and Gene Shively regarding the U.S. addiction epidemic and a healing path forward.
And finally, here is a video posted on the Kentucky Harm Reduction Coalition’s Facebook page with me discussing, what else? – Harm Reduction.
We interviewed board member and addiction specialist Dr. James Murphy on all things addiction, harm reduction, and the opioid epidemic. Give it a watch and spread the word – together we can break the stigma!
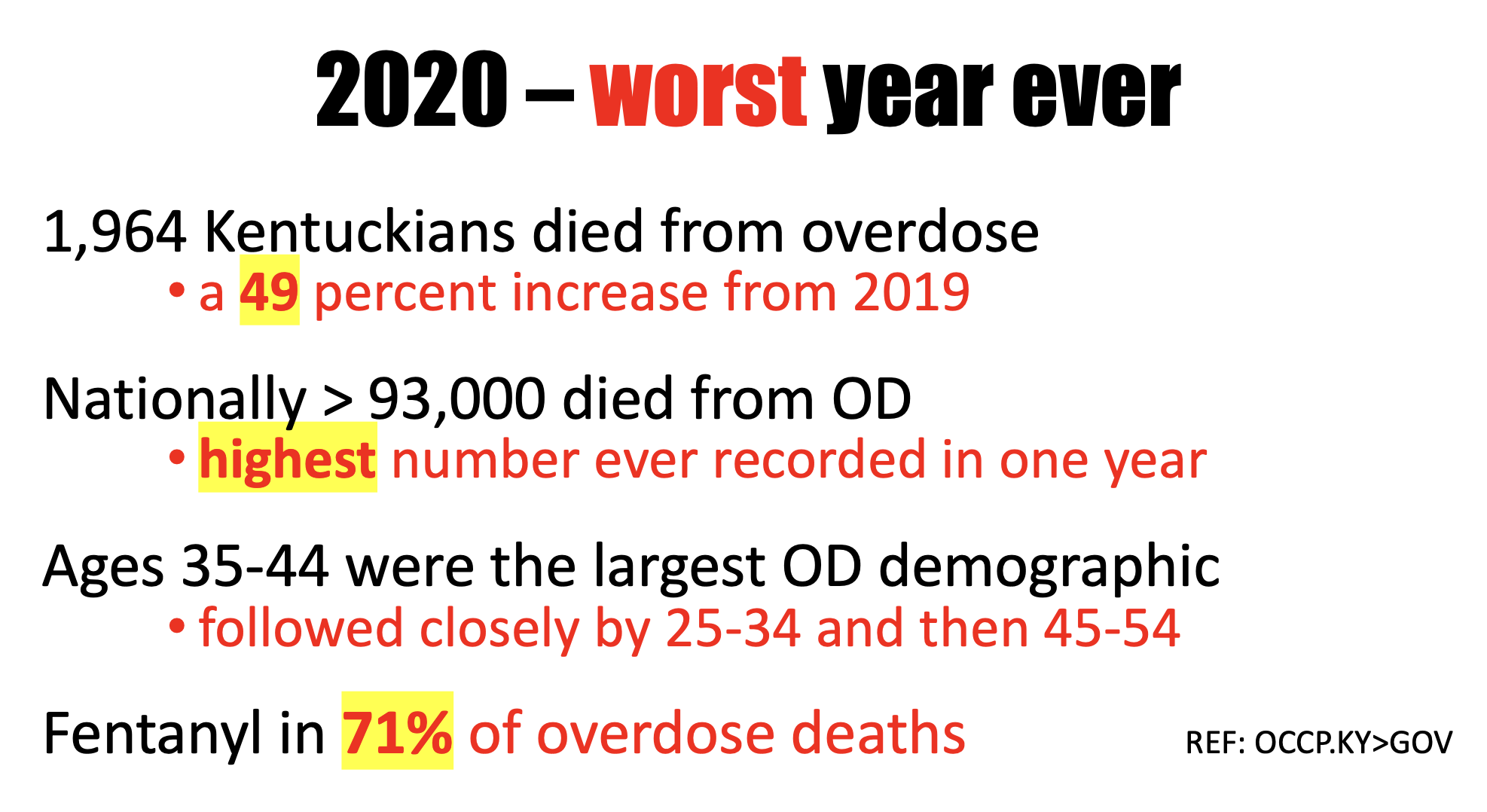
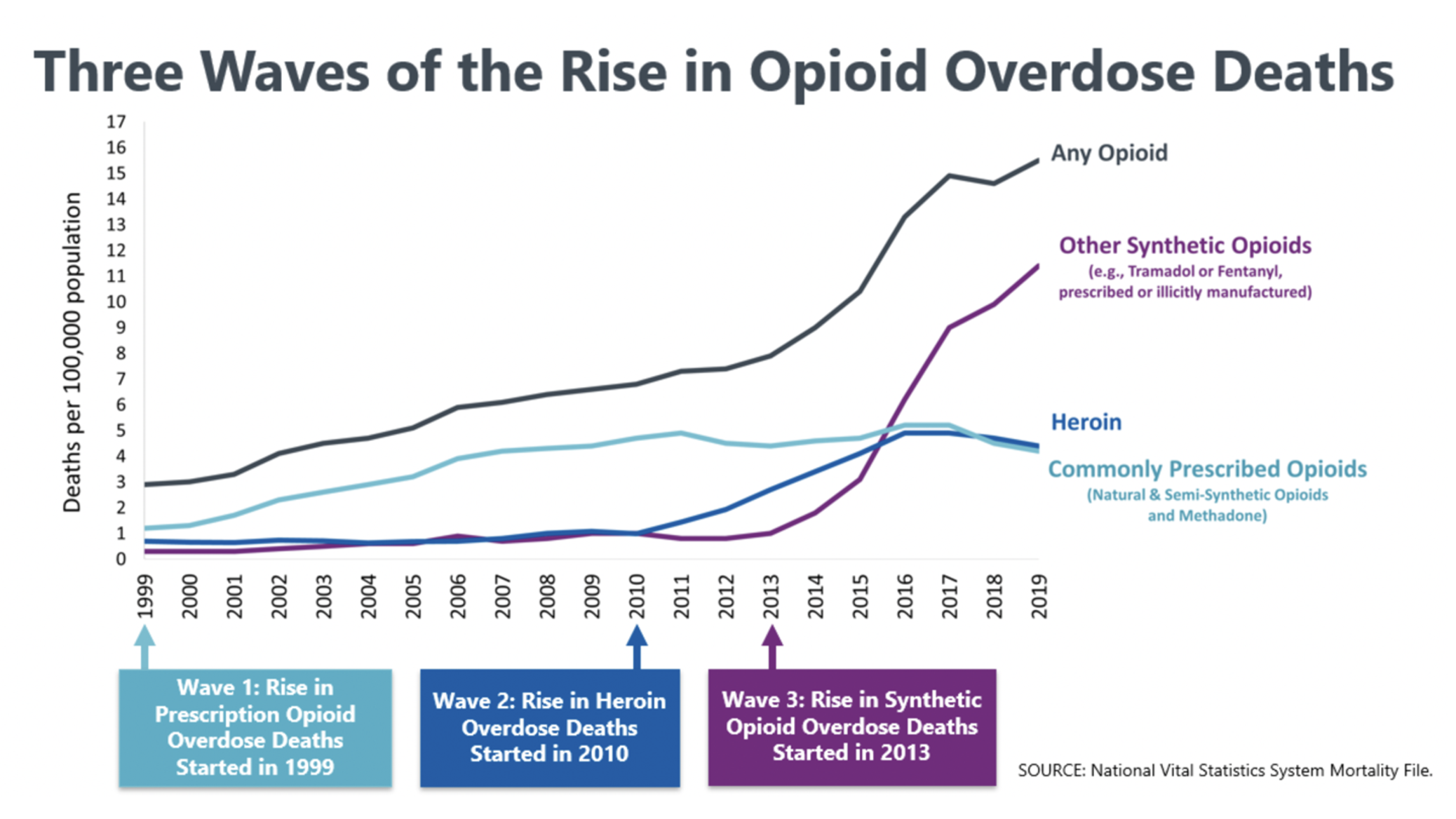
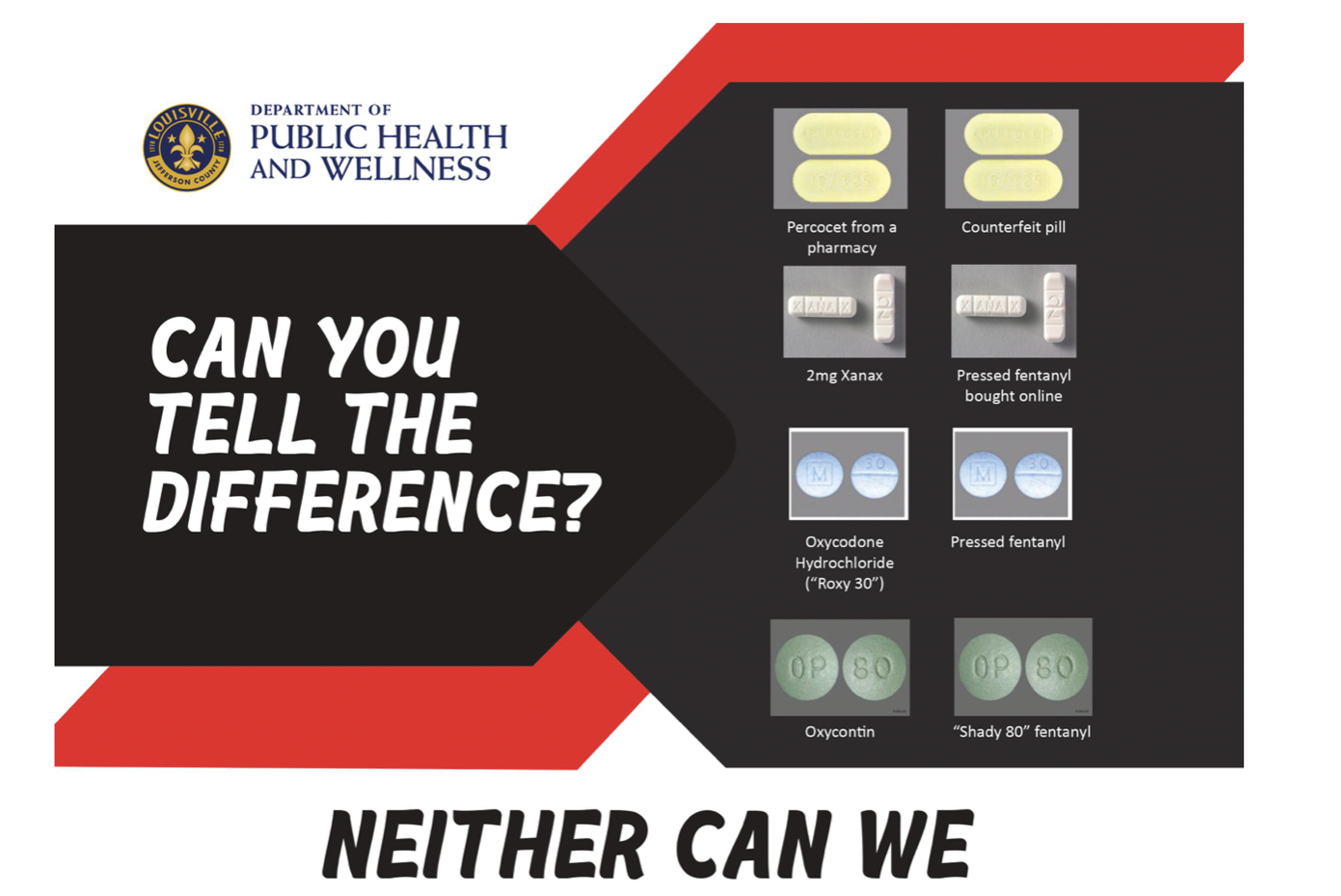
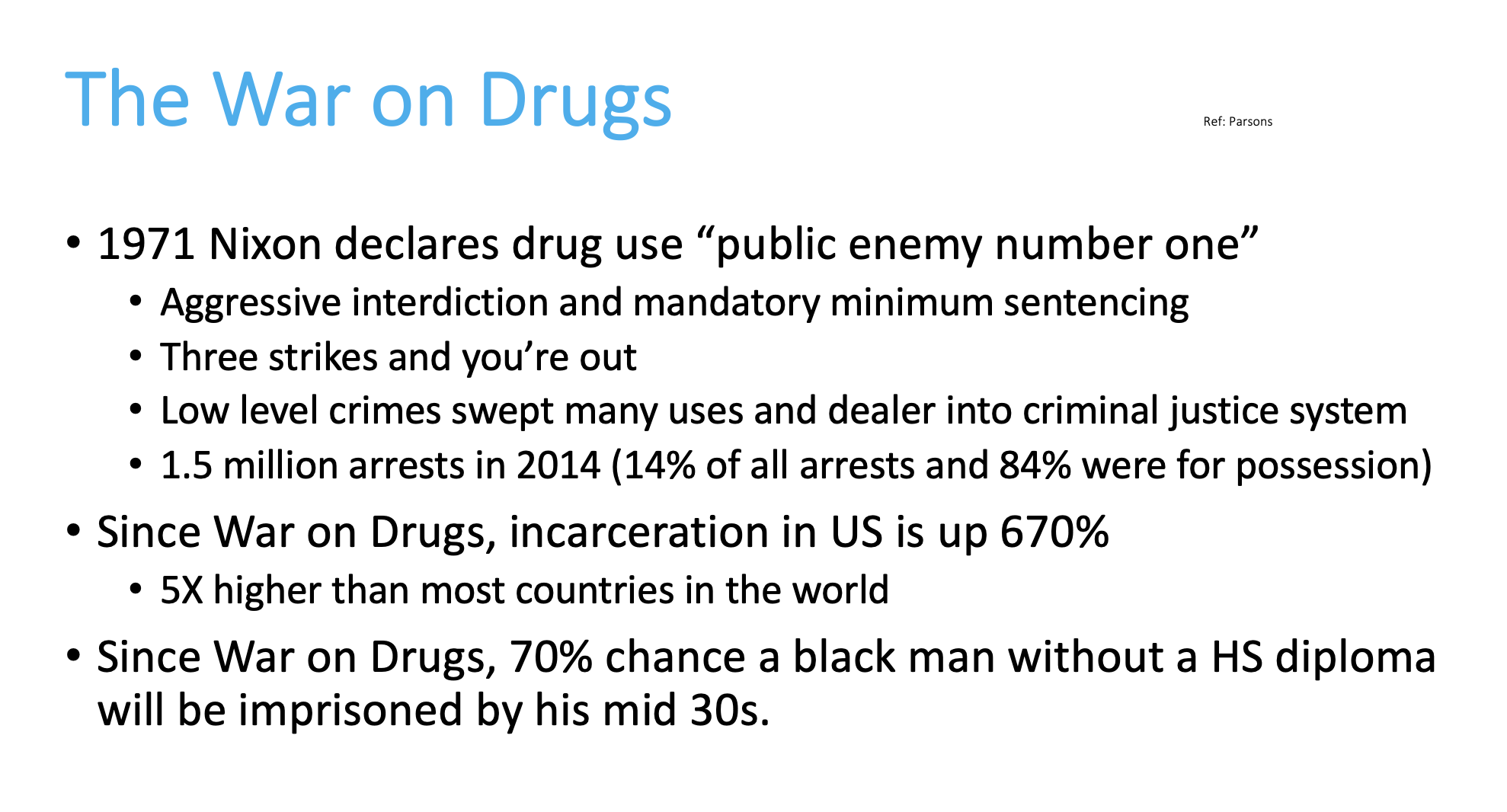
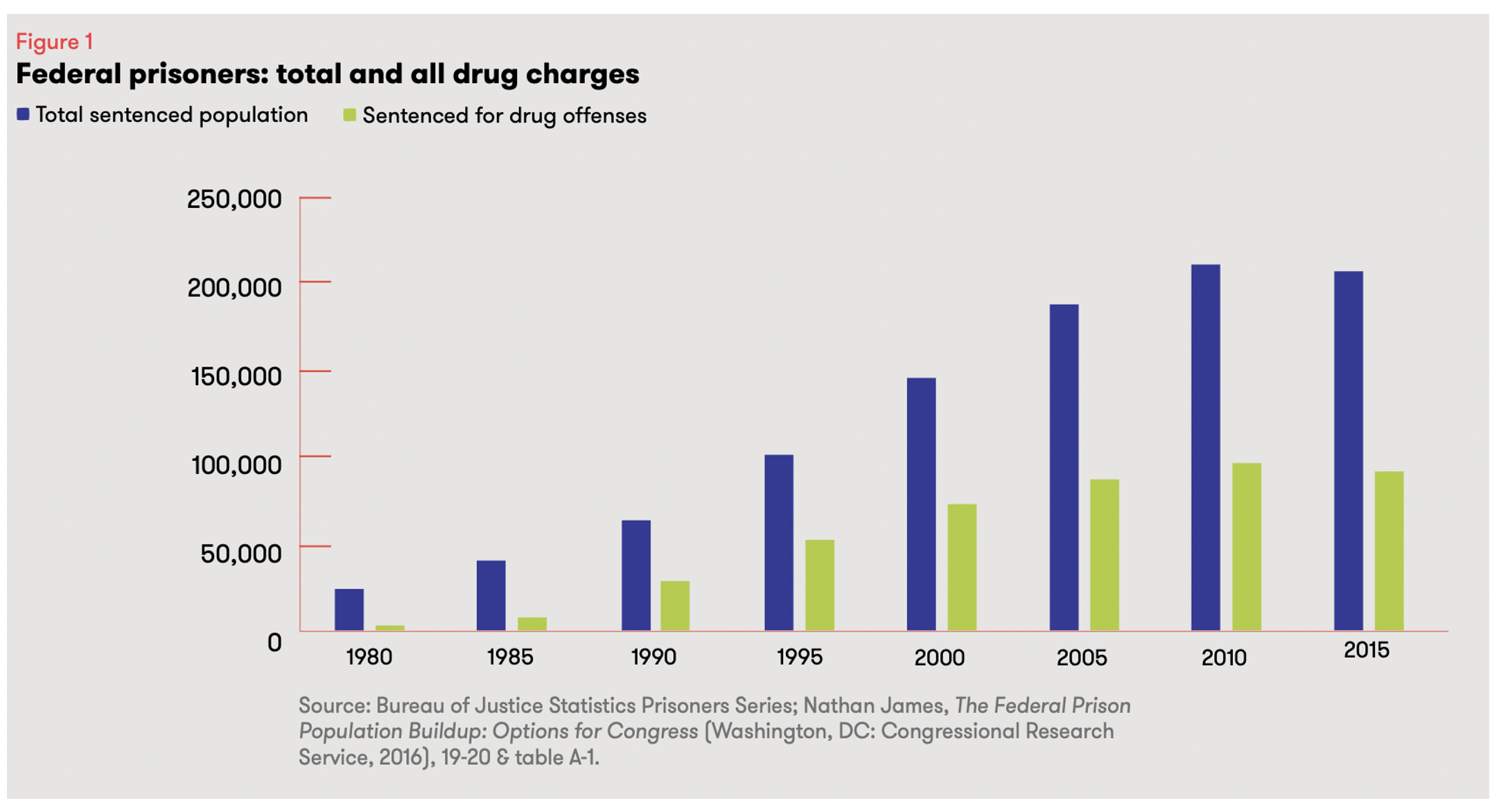
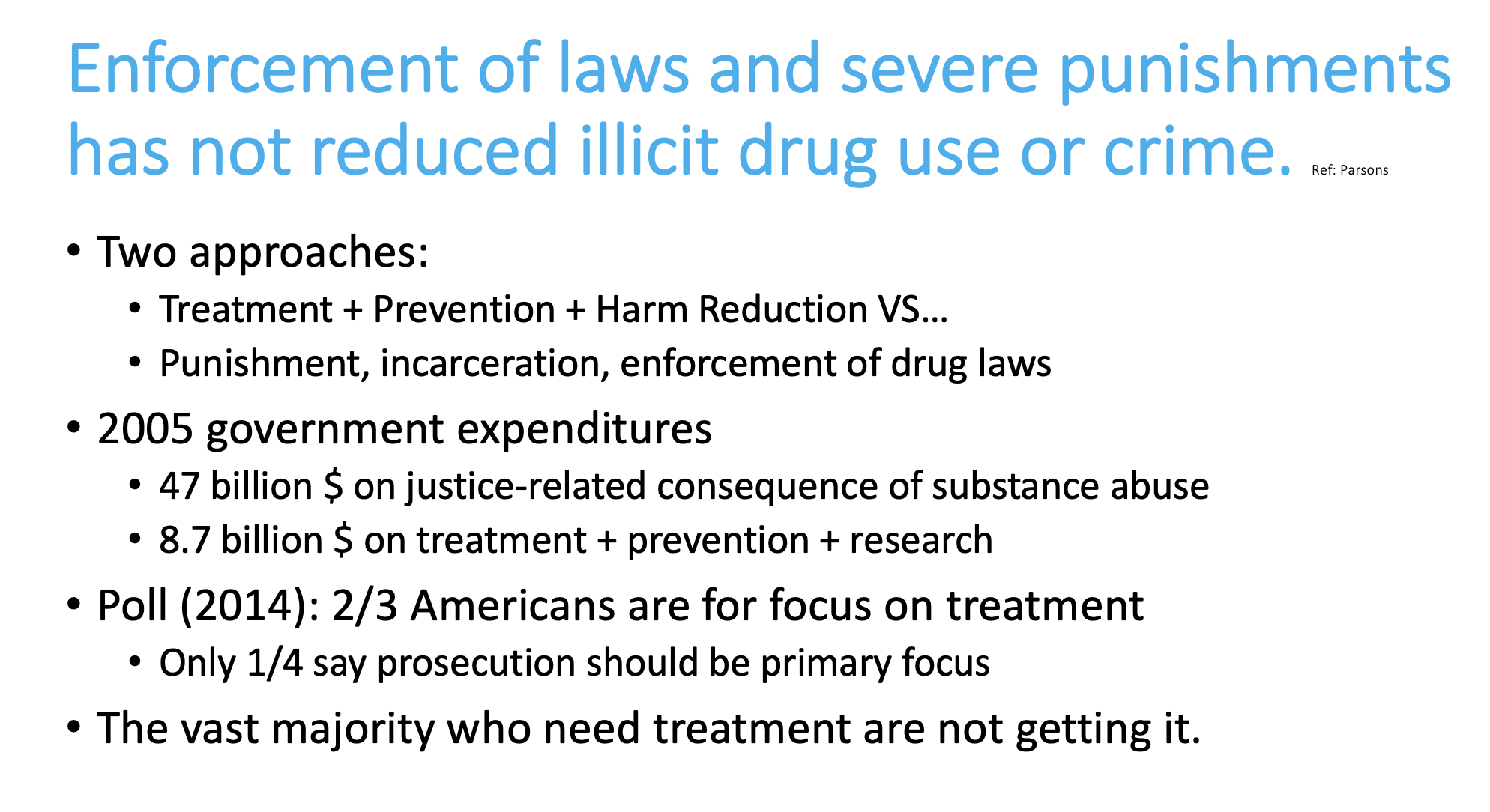
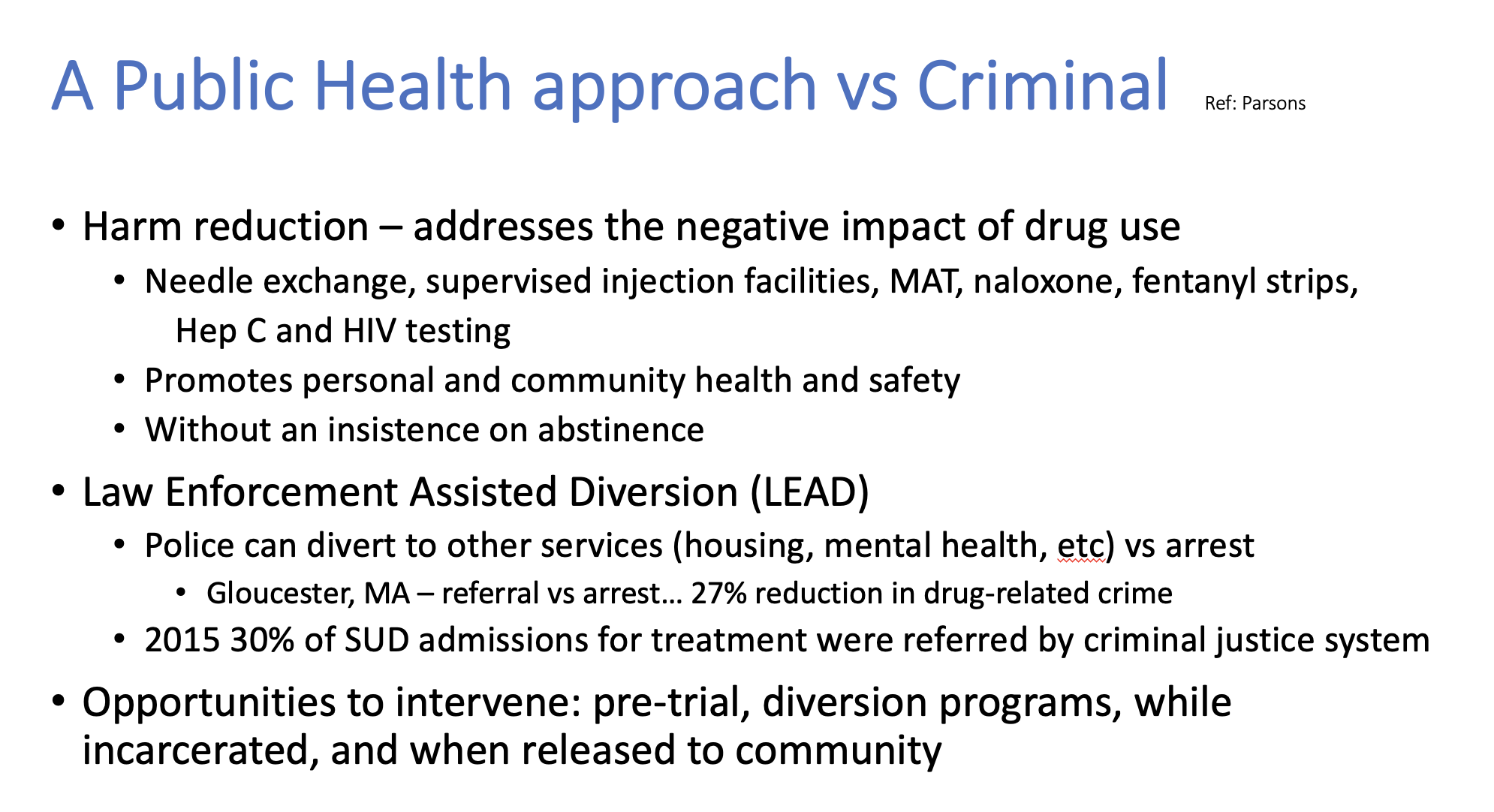
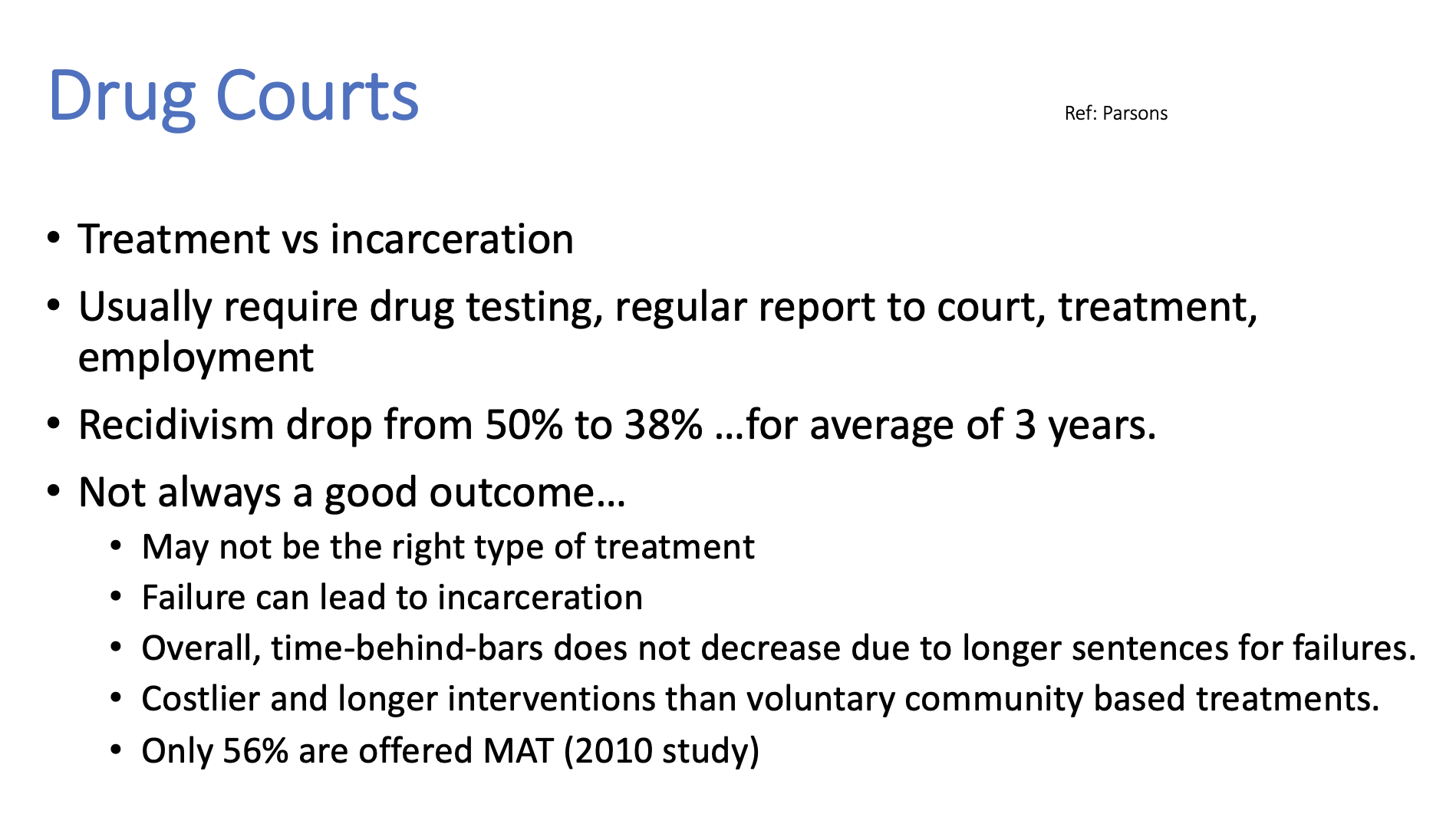
On June 13, 2022, I had the pleasure of presenting on the topic of MAT, i.e., Medication Assisted Treatment, or more recently known as MOUD, Medication for Opioid Use Disorder. Here is a selected portion of my slides, with some recommended references at the end. I sincerely appreciate being asked to give this presentation to such a wonderful and vital group of people serving our community and our justice system. It was an honor to be there with them for their Annual Public Defender Education Conference.
• Parsons, Jim: Minimizing Harm: Public Health and Justice System Responses to Drug Use and the Opioid Crisis by Jim Parsons. Vera Evidence Brief. December 2017
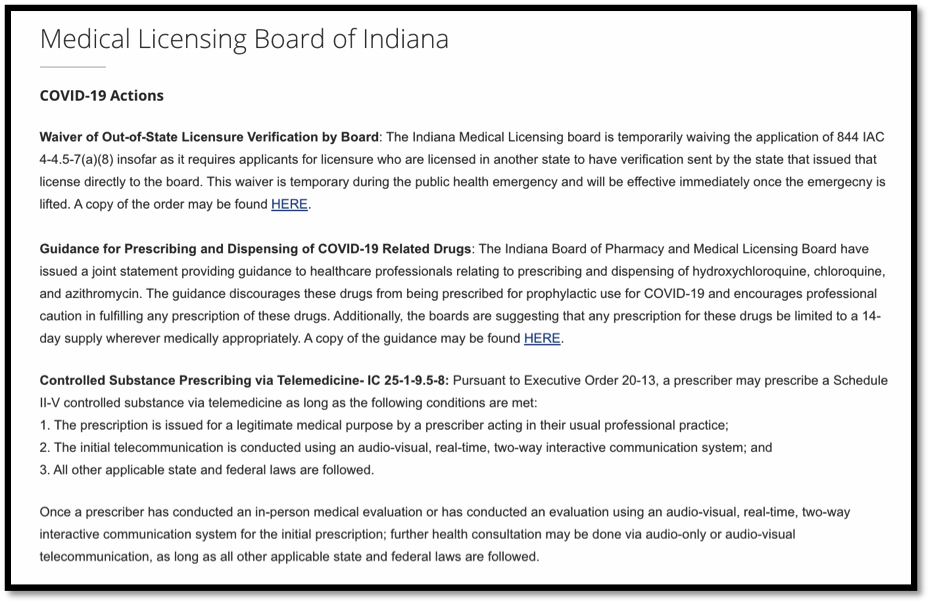
Once a prescriber has conducted an in-person medical evaluation or has conducted an evaluation using an audio-visual, real-time, two-way interactive communication system for the initial prescription; further health consultation may be done via audio-only or audio-visual telecommunication, as long as all other applicable state and federal laws are followed. (LINK: https://www.in.gov/pla/medical.htm)
I AM CERTAIN I SPEAK FOR MOST OF THE PROVIDERS, CITIZENS, AND PATIENTS OF INDIANA WHEN I SAY “THANK YOU” FOR THIS NECESSARY ACTION.
I am a New Albany, Indiana physician with an urgent plea. During the COVID-19 emergency, Indiana must allow prescribers to treat pain patients on opioids via audio-only telemedicine. Currently the requirement is for audio-visual telemedicine.
On March 6, 2020, Indiana declared a state of emergency due to COVID-19. As a result, extraordinary measures have been taken to allow patients to shelter in their homes. However, many chronic pain patients, among the most vulnerable to the SARS-CoV-2 Coronavirus, are still required to have in-person face-to-face visits with prescribers in order to receive a prescription for a controlled substance. This is because, although Indiana now allows audio-visual telemedicine for follow-ups, the state does not allow audio-only telephone calls to serve as telemedicine for controlled substance follow-up visits.
This has to change immediately.
We know that many people, especially the elderly, do not have access to audio-visual telecommunication. However, everyone has a telephone. Therefore, Indiana practitioners must be allowed to conduct audio-only telephone follow ups when prescribing controlled substances for their patients, especially patients who have previously had an in person examination. As it stands now, to prescribe an opioid via telemedicine, the Indiana Professional Licensing Agency still includes a requirement that: “The telecommunication is conducted using an audio-visual, real-time, two-way interactive communication system.”
Indiana has fallen dangerously behind the curve on this issue.
For example, look to the DEA’s COVID-19 Prescribing Guidance, which has been updated “to allow DEA-registered practitioners to prescribe controlled substances without having to interact in-person with their patients.” Specifically, the DEA now allows prescribers who have “previously examined the patient in person” to “conduct any needed follow-up evaluation by any method: in person, telemedicine, telephone, email, etc.”
And the American Medical Association’s “COVID-19 policy recommendations for OUD, pain, harm reduction” could not be more clear: “For patients with chronic pain, waive testing requirements and in-person counseling requirements for refills; allow for telephonic counseling to fulfill state prescribing and treatment requirements.”
In these extraordinary times, we must do everything in our power to ensure that all patients can access care remotely when at all possible. And for our patients with chronic pain on opioid therapy, the extreme stress from withdrawal or fear of withdrawal must be prevented or else we shall see increased and unnecessary morbidity and mortality amongst our citizenry. When patients are forced to leave their safe homes for face-to-face visits with providers, they imperil their lives, the lives of healthcare workers, and the lives of their community.
Audio-visual telemedicine, despite the perceived advantages as compared to a simple telephone call, is not feasible for many vulnerable Hoosiers. Indiana must join with the DEA, the AMA, and numerous other private and government organizations and immediately allow providers to remotely treat patients, for whom controlled substances are necessary, via any appropriate method, including audio-only telecommunication.
Thank you for your service to Indiana and thank you for taking the time to read this e-message. As soon as I hit “send” I will be on the telephone with my patient, Judy, who is 73, crippled with unimaginable arthritis, sheltering in her home, and anxiously waiting for her doctor to call. I have provided you my personal cell phone number in case you or someone on your staff would like to call me. I must apologize in advance, however, if the line is busy. As you well know, these are extraordinary times.
Respectfully,
James Patrick Murphy, MD
Medical Director, Murphy Pain Center, New Albany, IN
Assistant Clinical Professor, University of Louisville School of Medicine
Past-president, Greater Louisville Medical Society
Member, American Medical Association Pain Care Task Force
Where a prescription for a controlled substance is issued by means of the Internet, the CSA (as amended by the Ryan Haight Act) requires that such prescription involve at least one in-person medical evaluation, with limited exceptions. After conducting one in-person medical evaluation, a practitioner may thereafter prescribe controlled substances by means of the Internet or via telephone.
A verbal response to my question (see above) was transmitted during the Q&A portion of the Indiana State Department of Health Provider Webcast on April 3, 2020 and was encouraging:
Yes, we are doing this. We are putting together all the waivers that are done into a package and as soon as all the right people approve that will be done. So we heard you. I brought your question last week to the powers that be and they agree. So we’re working on that.
Lindsay Weaver, MD, FACEP, Chief Medical Officer, Indiana State Department of Health
DoctorJamesMurphy: Just to be clear, the information on the slide you posted today regarding controlled substances prescribing does not allow for audio-only telephone calls. The DEA specifically allows for audio-only telephone calls. Kentucky allows this. We are behind the curve on this. We need this in Indiana. Can you comment on the progress made in getting this done?
And here was the answer that Dr. Weaver recited on air:
So this again is a question about audio-only telephone calls. So I spoke specifically with our group about this and they did feel like it allowed for audio-only telephone calls. So I don’t know where the miscommunication is. I think there probably is another point to that waiver or that order that wasn’t included in that slide. If you just want to go ahead and send you name, then we can follow up with you or your email address. [Addendum: I immediately sent my email address]
Here is what I believe to be the miscommunication:
Dr. Weaver’s slide says this:
This slide indicates that Executive Order 2020-13 allows for “using a real-time, two-way interactive communication system.” This would appear to include audio-only telephone calls. But wait…
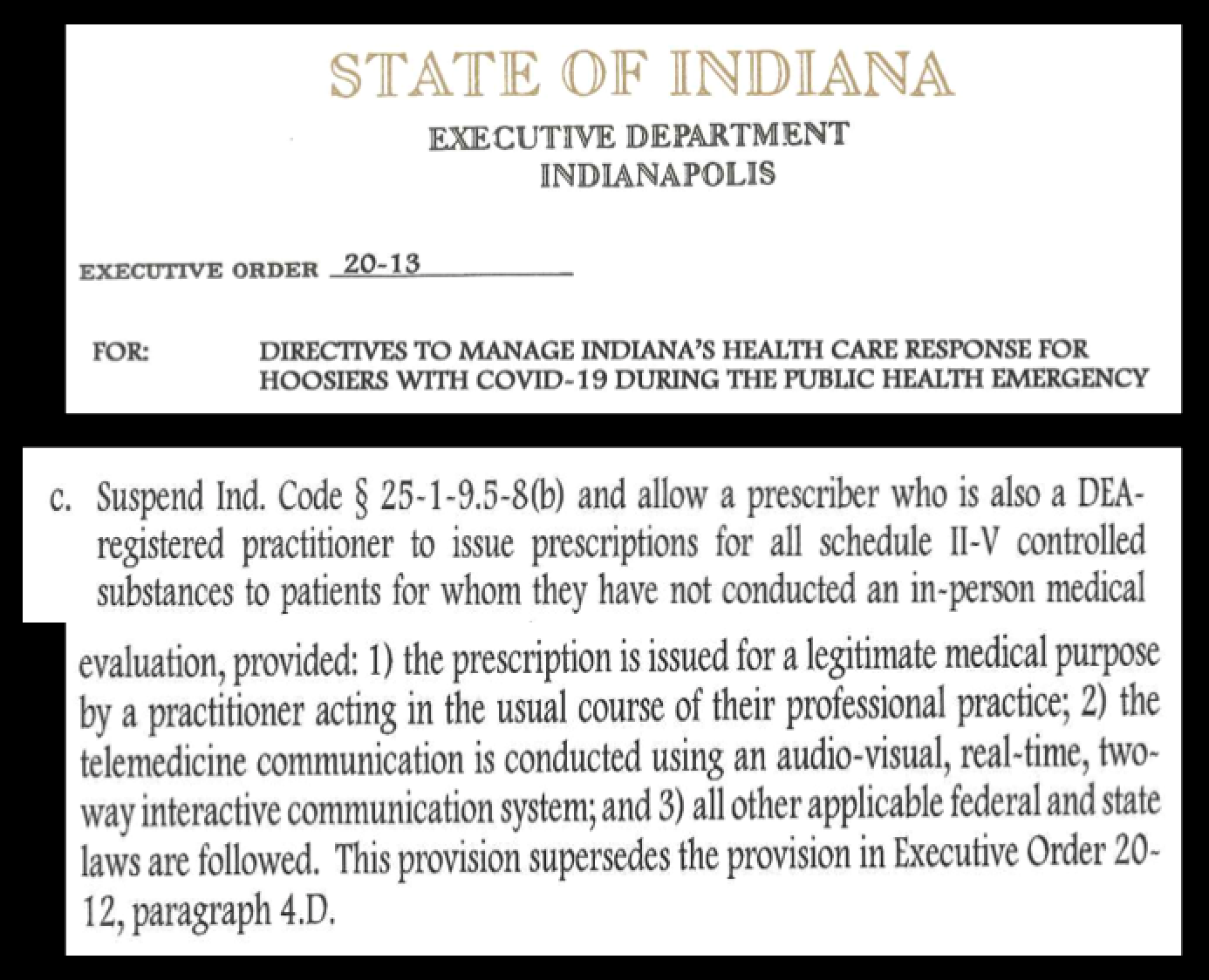
Dr. Weaver’s slide is not consistent with what Executive Order 2020-13 actually says, see below:
And there is more to the story… Executive Order 20-13 also says this:
In other words, Executive Order 20-13 seems to lift the prohibition against audio-only telemedicine by amending Indiana’s definition of telemedicine to include audio-only phone calls. Here is actual language from Indiana Code 25-1-9.5-6 that Executive Order 20-13 amends:
Therefore, it would seem that telemedicine in Indiana might now include “audio-only communication.”
So, as of 4:30 pm on April 9, 2020 here is where I believe this stands:
The slide presented today from Dr. Weaver, acting as an agent of the Indiana Department of Health, would appear to give a green light to audio-only telephone calls for issuing a controlled substance. But Dr. Weaver’s slide references Executive Order 20-13 that clearly does not say that audio-only telephone calls are sufficient. Where did Dr. Weaver get the verbiage for her slide?
And the COVID-19 updates to the the Indiana PLA website only references the previous Executive Order 20-12, which, like Executive Order 20-13, does not give the “OK” for audio-only telephone calls.
On top of that, the Indiana prescribing regulations, which no one is mentioning, still mandate a face-to-face visit (i.e. no mention of a telemedicine option) at least every four months.
From my non-lawyer, not offering legal advice, physician taking care of patients day in and day out point of view, it seems that somewhere in this cacophony of regulations, orders and pronouncements there is probably enough leeway to allow Indiana prescribers to go ahead and act in the best interest of their patients.
Dr. Lindsay Weaver is a board-certified Emergency Medicine physician engaged in battling the defining medical crisis of our time. She is doing an admirable job. And, with regards what the regs and the laws say we can and cannot do when prescribing controlled substances, she and I can totally agree on this…
To be valid, a prescription for a controlled substance must be issued for a legitimate medical purpose by a practitioner acting in the usual course of professional practice.
Importantly, the DEA Practitioner’s Manualgoes on to say:
Federal courts have long recognized that it is not possible to expand on the phrase “legitimate medical purpose in the usual course of professional practice” in a way that will provide definitive guidelines to address all the varied situations physicians may encounter.
Based on my research, terms like “legitimate medical purpose” and “usual course of professional practice” are not found in medical textbooks, nor are they taught in medical schools. It does not seem to be necessary. It is intuitive to physicians what we do and why we do it.
I am simply not comfortable with such a vital phrase remaining so inscrutable. And as a physician, I feel the dearth of clarity surrounding those ten words places all physicians, including myself, at risk. Consequently, this physician set out on a journey to “define thyself.”
The following (with links to references) represents a work in progress that, with help from numerous colleagues, wordsmiths, legal experts, patients, friends, lay people and trusted advisors, comprises my current best effort at expanding upon:
Legitimate medical purpose in the usual course of professional practice
In essence, for a duly licensed M.D or D.O. physician practicing medicine in the United States, this phrase from the DEA Practitioner’s Manual corresponds to a generally accepted process that, in the context of a patient-physician relationship, can correctly be expanded to mean: a science-based, moralart of caring wherein a physician serves a patient’s medical needs, primarily, by accessing and evaluating information that is utilized by the physician in deriving a clinical assessment, leading to the physician formulating a plan of care. With intent to mitigate harm to the patient, intent to provide benefit to the patient, intent to respect the patient’s right to autonomy, and intent to be mindful of how consequences might affect others, the physician in this course of practice exercises judgment that is considerate of scientific evidence, judgment that is reasoned by the physician to be in accord with standards in the field of medicine, and judgment that is born out of the physician’s knowledge, observations and intuition.
James Patrick Murphy, MD
First draft: 1/17/2020; most recent revision: 2/22/2020