201 KAR 9:270 departs from acceptedstandards by imposing non-individualized requirements across multiple aspects of care, including
treatment initiation,
setting,
dosing,
formulation,
dispensing intervals,
co-prescribed medications,
drug and laboratory testing,
counseling and behavioral requirements,
consultations,
documentation, and
responses to perceived noncompliance.
These requirements delay, disrupt, or block care and impose disproportionate burdens on individuals with OUD, particularly those with transportation issues, housing instability, employment disruption, or childcare responsibilities.
disruption of care for patients with significant physical disabilities;
delays or denials for patients receiving other medically necessary medications;
delayed initiation or continuation due to mandatory specialist consultations;
avoidance of treatment due to perceived regulatory risk;
treatment interruption due to transportation, housing, or cost barriers; and
inability to initiate buprenorphine in emergency, acute care, or unhoused settings due to regulatory or institutional constraints.
The regulatory burden also deters physicians from providing addiction treatment in Kentucky and reduces clinician participation statewide.
The 2023 elimination of the federal X-waiver requirement under the Controlled Substances Act, together with the 2024 Federation of State Medical Boards’ statement affirming access to evidence-based treatment for opioid use disorder, further undermines the justification for the restrictive requirements imposed under 201 KAR 9:270, which are not aligned with prevailing national standards of care. These restrictions appear unnecessary to the safe regulation of buprenorphine given national standards supporting individualized clinical judgment in MOUD treatment.
During a recent state regulatory review, the American Medical Association, American Society of Addiction Medicine, Kentucky Society of Addiction Medicine, and American Psychiatric Association advised that failure to sufficiently amend 201 KAR 9:270 could undermine Kentucky’s response to the opioid crisis.
The Legal Action Center and Kentucky Equal Justice Center further stated the regulation may have a discriminatory effect on individuals with OUD by limiting access to evidence-based treatment based on stereotypes and assumptions rather than clinical justification, and may interfere with providers’ ability to deliver care consistent with ADA requirements.
A September 2022 Kentucky Opioid Response Effort (KORE) flier reported that buprenorphine reduces illicit opioid use and fatal overdose by over 50%. However, only approximately 20% of the estimated 150,000+ Kentuckians with OUD receive MOUD. Given this prevalence, 201 KAR 9:270 affects a substantial population that may be protected under the ADA. By conditioning access to buprenorphine on blanket regulatory requirements rather than individualized clinical judgment, the regulation creates statewide barriers to medically necessary care across settings and regions.
I respectfully request that the Department investigate 201 KAR 9:270 and consider enforcement action to remedy potential ADA violations. I will also submit supporting documentation by email.
A broad coalition of healthcare, public safety, and recovery organizations across Kentucky has come together to back HB 153 / SB 82, legislation that removes outdated barriers to evidence-based treatment for opioid use disorder. The coalition includes advocacy groups, recovery organizations, and prominent voices such as the Kentucky Sheriffs’ Association, Kentucky Society of Addiction Medicine, Greater Louisville Medical Society, Kentucky Nurses Association, and Appalachian Regional Healthcare. This unified support highlights the urgent need to expand access to proven treatments and save lives in communities across the state.
Note: The letter is still open for signatures. Email James Patrick Murphy MD at jpmurphy.mpc@gmail.com to join the support for HB 153 / SB 82.
Updated: April 22, 2026
Dear Honorable Members of the General Assembly:
The undersigned organizations, representing more than twenty-four law enforcement, medical societies and patient advocacy groups, respectfully request your co-sponsorship and support for HB153 / SB82. This important legislation would remove harmful regulatory barriers that unnecessarily limit access to the medication buprenorphine. As a result of these restrictions, too few Kentuckians with opioid use disorder (OUD) receive this life-saving medication at great cost to the people of our Commonwealth.
The ongoing overdose crisis demands a bold response which utilizes all policy tools to support our families, friends, and communities. Buprenorphine is an U.S. Food and Drug Administration-approved medication for the treatment of OUD and has been proven to significantly improve health outcomes for people with OUD.[i] Specifically, buprenorphine treatment is associated with reduced overdose deaths and criminal activity.[ii][iii] Further, evidence suggests that expanding access to this medication is a cost-effective strategy that would save both lives and taxpayer money.[iv]
In fact, the U.S. Department of Health and Human Services recently added all forms of medications for opioid use disorder (MOUD), including buprenorphine, as preventive services eligible for federal funding through the Administration for Children and Families under President Trump’s recent Executive Order: Addressing Addiction Through the Great American Recovery Initiative. Supporting HB153 / SB82 would help Kentucky follow the Trump Administration’s lead in promoting evidence-based treatment and recovery for more Americans with OUD.
Further, Kentucky’s special regulations governing buprenorphine are burdensome, flawed, and unnecessary. Last year, leading state and national medical societies identified several deficiencies with the regulations that remain unaddressed.[v]As such, the General Assembly now has an opportunity to correct course and remove this deficient regulation altogether. Notably, if HB153 / SB82 is enacted, buprenorphine will be regulated in the same manner as other Schedule III controlled substances. Therefore, HB153 / SB82 is a common-sense effort to simplify our regulatory scheme and return treatment decisions to clinicians and patients.
Opponents of this legislation warn that removing special regulations on buprenorphine would increase the risk that this medication is diverted. However, evidence suggests that most people use any diverted buprenorphine to self-treat withdrawal and more strictly regulating buprenorphine may actually increase diversion risk.[vi]As such, we must work to ensure that evidence-based treatment for OUD is more accessible in Kentucky. Enacting HB153 / SB82 is a significant step towards accomplishing that goal.
Ultimately, HB153 / SB82 is sensible legislation that would reverse flawed regulations and promote treatment, remission, and recovery for more Kentuckians. As such, we are proud to support this legislation and respectfully urge your co-sponsorship and support for its passage soon. Thank you for your consideration.
Sincerely,
Signatories in Support of HB 153 / SB 82 (Updated April 22, 2026):
Appalachian Regional Healthcare officially supports HB 153 / SB 82 – ARH, with more than 1,300 providers across its multi-state system, is the largest provider of care and the single largest employer in southeastern Kentucky.
Leadership representing over 30,000 first responders and frontline workers—including Louisville EMS and MetroSafe— supports HB 153 / SB 82.
Kentucky Professional Fire Fighters, representing forty-three fire fighter and EMS unions throughout Kentucky, officially supports HB 153 / SB 82.
Kentucky Firefighter’s Association, serving and promoting the interests of all firefighters in the Commonwealth of Kentucky, officially supports HB 153/ SB 82.
The Greater Louisville Medical Society independently expressed strong support for HB 153 / SB 82 (full letter to the General Assembly attached below), stating:
HB 153 / SB 82 is sensible legislation that would update flawed regulations and promote treatment, remission, and recovery for more Kentuckians. We are proud to support this legislation and respectfully urge your co-sponsorship and support for its passage soon.
Consistent with the goals of HB 153 / SB 82, the following organizations have previously called for the revision or repeal of Kentucky’s buprenorphine regulation, 201 KAR 9:270:
In August 2025, the Kentucky Medical Association (KMA) House of Delegates adopted a range of resolutions submitted by the Greater Louisville Medical Society (GLMS). Of particular note, the buprenorphine-related resolutions align closely with the goals of HB 153 / SB 82:
Buprenorphine Saves Lives: Recognized as a life-saving, evidence-based treatment for opioid use disorder, reducing overdose deaths.
Remove Barriers: Calls for eliminating unnecessary regulatory (i.e., KBML Regulation 201 KAR 9:270) and insurance obstacles that limit patient access.
Protect Physician Judgment: Safeguards doctors prescribing buprenorphine within accepted standards of care.
Chronic Pain Care: Supports evidence-based use of buprenorphine—including off-label applications—for appropriate patients.
Expert Input: Urges the Kentucky Board of Medical Licensure to consult widely with clinicians and subject matter experts when updating regulations.
These resolutions demonstrate GLMS and KMA’s commitment to expanding access to effective, evidence-based treatments and improving patient outcomes across Kentucky.
On August 1, 2024, a petition delivered to the Kentucky Board of Medical Licensure called for removing barriers to buprenorphine treatment and creating a transparent review process—steps fully aligned with HB 153 / SB 82. Both the petition and the bill aim to:
• Expand access to evidence-based treatment for opioid use disorder • Support patient-centered care • Help Kentucky physicians save lives
The 350+ petition signers include prominent voices affiliated with—although not necessarily representing—the following organizations:
Medical & Academic Institutions: • University of Louisville School of Medicine & Class of 1985 alumni • University of Kentucky College of Medicine & UK HealthCare • UofL Health • Penn State College of Medicine • Stanford University School of Medicine • University of Central Florida • University of Pennsylvania • University of Colorado School of Medicine • Johns Hopkins University • University of New Mexico • Robley Rex VA Medical Center
Medical Societies & Associations: • Greater Louisville Medical Society (GLMS) • Kentucky Society of Addiction Medicine (KYSAM) • American Society of Addiction Medicine (ASAM) • American Academy of Addiction Psychiatry • Kentucky Medical Association (KMA) • American College of Obstetricians & Gynecologists (ACOG), KY Section
Hospitals, Recovery & Behavioral Health Organizations: • St. Elizabeth Physicians & Journey Recovery Center • Brighton Recovery Center • Norton Healthcare • Baptist Health Louisville • Appalachian Regional Healthcare • BrightView Health & Brightview Addiction Centers • Alteri Behavioral Health • East Kentucky Rehabilitation Centers • Healing The Children KY • Discover Recovery, LLC • Bluegrass Care Navigators • Beacon House Aftercare • Ultimate Treatment Center, Ashland KY
Clinical Experts & Practitioners: • Addiction medicine physicians and specialists (MD, DO, FASAM) • Psychiatrists & psychiatric nurse practitioners (PMHNP-BC) • Pain management specialists & anesthesiologists • Internal medicine, family medicine, OB/GYN, pediatrics, and palliative care physicians • Licensed clinical social workers (LCSW, LCADC) • Pharmacists, CRNAs, and other allied health professionals • Medical students, residents, and fellows from ULSOM and UK
Additional Stakeholders & Advocates: • Elected members of the Kentucky General Assembly • Patient advocates, concerned citizens, and bereaved family members • Military and public safety professionals • Attorneys, researchers, and public policy experts
Affiliations reflect the organizations of individual petition signers and do not imply official institutional endorsement.
[ii] Santo, T., Clark, B., Hickman, M., Grebely, J., Campbell, G., Sordo, L., Chen, A., Tran, L. T., Bharat, C., Padmanathan, P., Cousins, G., Dupouy, J., Kelty, E., Muga, R., Nosyk, B., Min, J., Pavarin, R., Farrell, M., & Degenhardt, L. (2021). Association Between Length of Buprenorphine or Methadone Use and Nonprescribed Opioid Use Among Individuals with Opioid Use Disorder: A Cohort Study. JAMA Psychiatry, 78(9), 979. https://doi.org/10.1001/jamapsychiatry.2021.0976
[iii] Molero, Y., Zetterqvist, J., Binswanger, I. A., Hellner, C., Larsson, H., & Fazel, S. (2018). Medications for Alcohol and Opioid Use Disorders and Risk of Suicidal Behavior, Accidental Overdoses, and Crime. American Journal of Psychiatry, 175(10), 970–978. https://doi.org/10.1176/appi.ajp.2018.17101112
[iv] Fairley, M., Humphreys, K., Joyce, V. R., Bounthavong, M., Trafton, J., Combs, A., Oliva, E. M., Goldhaber-Fiebert, J. D., Asch, S. M., Brandeau, M. L., & Owens, D. K. (2021). Cost-effectiveness of Treatments for Opioid Use Disorder. JAMA Psychiatry, 78(7), 767. https://doi.org/10.1001/jamapsychiatry.2021.0247
[vi] Rubel, S. K., Eisenstat, M., Wolff, J., Calevski, M., & Mital, S. (2023). Scope of, Motivations for, and Outcomes Associated with Buprenorphine Diversion in the United States: A Scoping Review. Substance Use & Misuse, 58(5), 685–697. https://doi.org/10.1080/10826084.2023.2177972
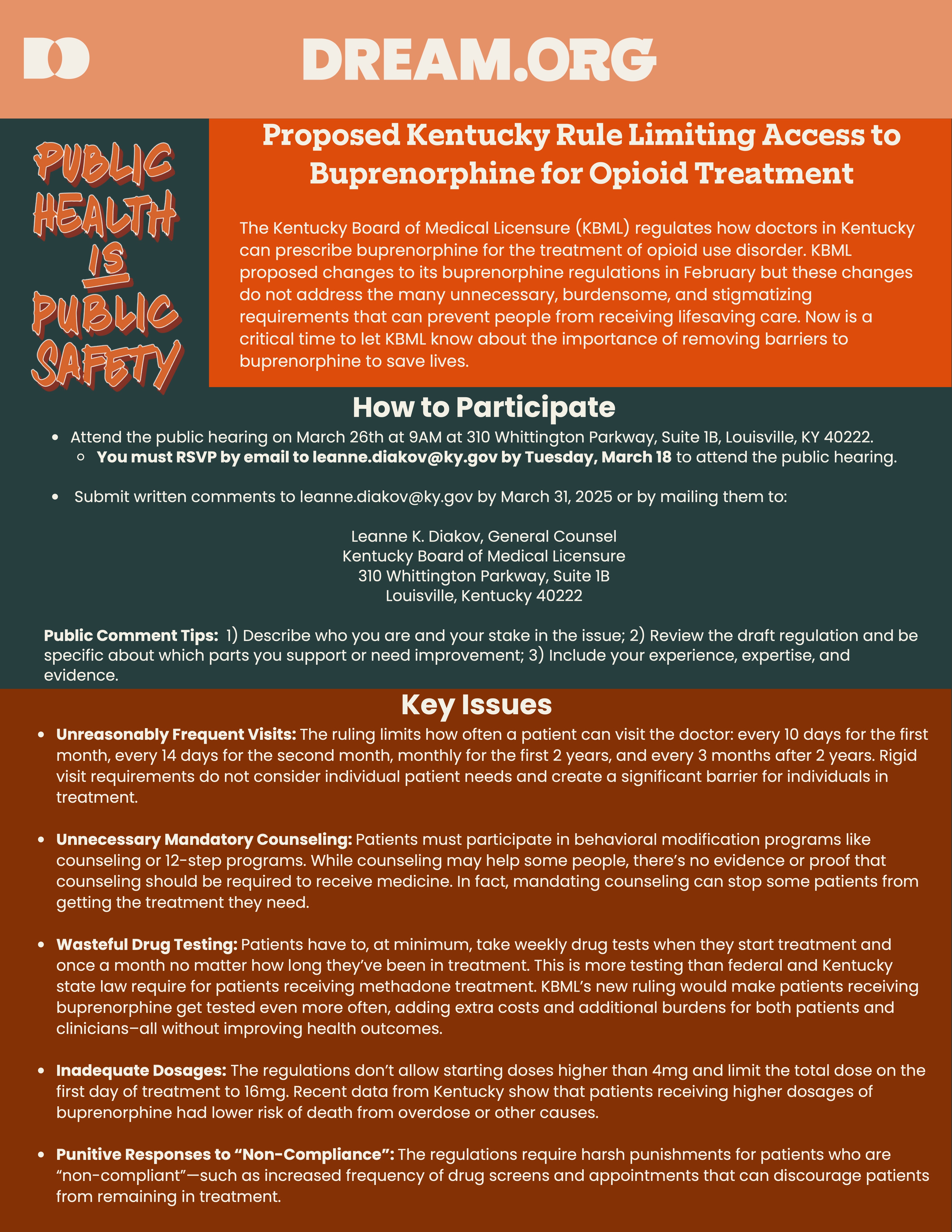
HERE’S THE LATEST: The Kentucky Board of Medical Licensure (KBML) filed their updated version of 201 KAR 9:270 (the buprenorphine regulation) and scheduled an in-person public hearing for March 26, 2025. However, KBML cancelled this hearing due to an overwhelming number of requests by speakers to be heard. KBML has now rescheduled the hearing for June 27, 2025, only this time it’s not in-person. It’s a Zoom meeting! They have not posted the link yet, so stay tuned and monitor the KBML website, link: https://kbml.ky.gov/Pages/index.aspx
Please mark your calendar for June 27th and spread the news. To review, below is a call to action from Dream.org sent prior to the cancelled March 26th hearing – NOW JUNE 27. The same issues are still at stake. Your voice is needed now more than ever! Even if you only Zoom in for thirty seconds. YOUR WRITTEN COMMENTS MATTER TOO! THANK YOU!
Dear Friends, Neighbors, and Colleagues,
Now is the time to take action! Your voice can make a difference in Kentucky. A simple email could help save lives. Here’s how: Send an email to the Kentucky Board of Medical Licensure (KBML) via
Leanne K. Diakov, KBML General Counsel at leanne.diakov@ky.gov
To make it easier, simply click on this LINK, where you’ll find a helpful brief to guide you in crafting and sending your email to leanne.diakov@ky.gov
NOTE: KBML HAS RESCHEDULED THE PUBLIC HEARING FOR JUNE 27, 2025, AND ARE ACCEPTING EMIALS AND WRITTEN COMMENTS THROUGH JUNE 27.
Tell KMBL that you do not support the proposed changes Kentucky’s buprenorphine regulation, and you believe Kentucky would be better served by eliminating the entire regulation known as 201 KAR 9:270.
The Kentucky Board of Medical Licensure (KBML) is nearing the final stages of updating the regulation 201 KAR 9:270, which governs the treatment of Opioid Use Disorder with buprenorphine in Kentucky. Even with the proposed changes, this regulation remains flawed and harmful, and KBML has yet to fully acknowledge the impact. You don’t have to take my word for it. Read it for yourself at https://apps.legislature.ky.gov/law/kar/titles/201/009/270/REG/
Unfortunately, KBML’s proposed amendments do not address the damaging, stigmatizing policies first introduced in 2015. But you still have time to help alter this course. Until JUNE 27, you can make your voice heard with an email to KBML.
Despite input from hundreds of specialists, caregivers, and concerned Kentuckians calling for significant revisions to this harmful regulation, KBML has moved forward with publishing insufficient amendments to their outdated regulations on buprenorphine prescribing. Sadly, these amendments do little to improve the situation and further create barriers for patients seeking this life-saving treatment.
Kentucky is out of sync with the rest of the country. While federal guidelines have simplified and streamlined buprenorphine prescribing in recent years, Kentucky remains one of the few states enforcing stricter, punitive measures. Kentucky’s buprenorphine regulation (and its proposed amendments) are not only unsupported by evidence but also contribute to an increase in overdose deaths by limiting access to care.
If 201 KAR 9:270 and its proposed amendments are allowed to proceed, Kentucky will miss the opportunity to align itself with thelatestscientificevidence, expertrecommendations, and current federal guidelines. Continuing with Kentucky’s flawed regulation will only result in more preventable overdose deaths in our state.
A ban on using buprenorphine-naloxone for chronic pain
It’s time to take action!
Now through JUNE 27, you have the opportunity to speak up on behalf of those struggling with opioid use disorder. Email your comments to:
Leanne K. Diakov, KBML General Counsel: leanne.diakov@ky.gov
At the end of this post, you’ll find a sample letter that you can modify to share your personal perspective, if you wish. Personalizing your message can make a big impact!
The Director of the National Institute on Drug Abuse stated that if everyone who needs buprenorphine could access it, overdose deaths could be reduced by half.
201 KAR 9:270 is a barrier preventing Kentuckians from accessing this life-saving medication.
And despite a tsunami of evidence proving the lifesaving effects of this medication, buprenorphine prescribing in Kentucky actually decreased last year! We must do better!
What more motivation do you need? Together, we can make a difference. Let your voice be heard!
Dr. Murphy is Kentucky’s Regional Director for the American Society of Addiction Medicine and is a founding member of the American Medical Association’s Substance Use and Pain Care Task Force. He serves as an Assistant Clinical Professor for the University of Louisville School of Medicine and is board-certified in Anesthesiology, Pain Management, and Addiction Medicine.
***SAMPLE TEXT***
To: Kentucky Board of Medical Licensure Attention: Leanne K. Diakov, General Counsel Email: leanne.diakov@ky.gov
RE: Public Comments on Proposed Amendments to 201 KAR 9:270
Dear Members of the Kentucky Board of Medical Licensure,
I am submitting my public comments on the proposed amendments to 201 KAR 9:270. Rather than addressing Kentucky’s overdose crisis, I am concerned that these proposed changes will only worsen the situation, creating additional barriers to care and limiting access to critical, lifesaving treatments. I respectfully urge the Board to prioritize evidence-based addiction treatment by rejecting these amendments and fully repealing this outdated and harmful regulation.
Expanding access to medications for opioid use disorder, such as buprenorphine, is crucial for reducing overdose deaths. Unfortunately, the proposed amendments directly contradict the guidance from several leading authorities, including the U.S. Department of Health and Human Services, the Drug Enforcement Administration, the Substance Abuse and Mental Health Services Administration, the National Institute on Drug Abuse, and the Federation of State Medical Boards, all of which support broader access to buprenorphine-based treatments. The restrictions outlined in 201 KAR 9:270 would be counterproductive and could exacerbate health disparities, especially within marginalized communities.
If these proposed amendments are enacted, 201 KAR 9:270 will continue to contribute to Kentucky’s tragically high overdose death rate. I fully support the concerns raised by the Kentucky Society of Addiction Medicine, which has reviewed the proposed changes and deemed them insufficient. In light of these concerns, I strongly advocate for the full repeal of 201 KAR 9:270.
Thank you for considering the potential impact of these amendments on the health and well-being of Kentuckians. I urge the Board to prioritize evidence-based addiction treatment by rejecting these amendments and fully repealing this outdated and harmful regulation.
Sincerely, [Your Name] [Your Credentials/Professional Title, if applicable]
Kentucky House Bill 788 (currently in committee) supports increased access to buprenorphine by empowering Kentucky’s providers to treat patients with evidence-based care. Check out this 9 minute video of Dr. Murphy’s recent testimony in Kentucky’s capital city: https://www.youtube.com/watch?v=3lILI0x4TXo
More and more people and organizations are joining this cause…
3/15/2025 UPDATE – For the time being, the ALARM ACT initiative has been merged with HB 788, which was filed by Representative Kim Moser in the Kentucky General Assembly. For more information check out the KYSAM advocacy HB 788 website: https://www.kysam.org/news
Kentucky House Bill 788 supports increased access to buprenorphine by empowering Kentucky’s providers to treat patients with evidence-based care. Check out this 9 minute video of Dr. Murphy’s recent testimony in Kentucky’s capital city: https://www.youtube.com/watch?v=3lILI0x4TXo
The salient issues remain consistent with the ALARM ACT initiative, thus I’m keeping this post on the website to provide historical context supporting our efforts to save lives.
ALARM Act one-page advocacy brief
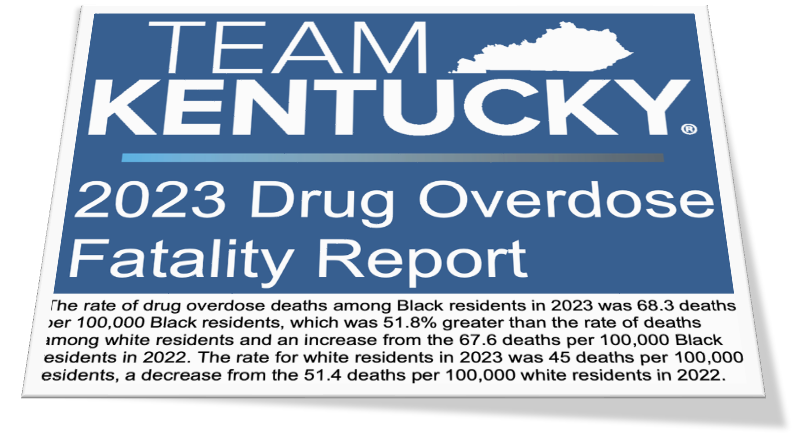
On average, FIVE Kentuckians die every day from overdose – about 2000 deaths per year.
• In sum, buprenorphine helps people achieve sustained recovery and lead healthy productive lives.
But there are barriersin the way of Kentuckians’ access to buprenorphine treatment. The barriers include: (1) stigma born of prejudice & misunderstanding, (2) unfounded fear of diversion, (3) excessive costs from unnecessary regulatory requirements, and (4) burdensome administrative hoops.
KY’s buprenorphine regulation 201 KAR 9:270 is a major regulatory barrier.
Frankly, the mandates in 201 KAR 9:270 are inconsistent with clinical evidence, expert opinion, or even the DEA – and even when 201 KAR 9:270 is repealed, the DEA will continue to regulate buprenorphine like any other schedule three controlled medication. But for now, 201 KAR 9:270 still exists and contributes to the fact that only1 in fivepeoplewho need treatment with buprenorphine can access the medication.
Can you imagine restricting treatment of cancer, diabetes, or any other disease in such a callous way?
The ALARM Act is backed by the Kentucky Society of Addiction Medicine, along with a vast majority of professional societies, scientists, scholars, medical school professors, physicians, caregivers, and countless other Kentuckians affected by the disease of opioid addiction. The ALARM Act repeals 201 KAR 9:270 and empowers Kentucky doctors to treat their patients with evidence-based medication, saving valuable healthcare resources and, most importantly, saving precious lives. Please support the ALARM Act.
More information can be found via the Kentucky Society of Addiction Medicine’s website: KYSAM.ORG
3/15/2025 UPDATE – For the time being, the ALARM ACT initiative has been merged with HB 788, which was filed by Representative Kim Moser in the Kentucky General Assembly. For more information check out the KYSAM advocacy HB 788 website: https://www.kysam.org/news
Kentucky House Bill 788 supports increased access to buprenorphine by empowering Kentucky’s providers to treat patients with evidence-based care. Check out this 9 minute video of Dr. Murphy’s recent testimony in Kentucky’s capital city: https://www.youtube.com/watch?v=3lILI0x4TXo
The salient issues remain consistent with the ALARM ACT initiative, thus I’m keeping this post on the website to provide historical context supporting our efforts to save lives.
On average, overdose kills five Kentuckians every single day.
There is something simple you can do today to help.
A brief call to your legislators, asking them to support the ALARM Act, could help save thousands of lives.
The ALARM Act is a legislative initiative aimed at improving access to buprenorphine – a lifesaving medication to treat opioid addiction – in fact, buprenorphine is our MOST EFFECTIVE measure to decrease overdoses and overdose deaths. The ALARM Act repeals regulation 201 KAR 9:270 – a decade-old KY law that severely hampers our doctors’ ability to prescribe buprenorphine.
Simply dial (800) 372-7181, and your message will be forwarded to your representatives.
You might say something to the effect of: Please help patients get the lifesaving medicine they need to treat addiction and prevent overdose deaths. Please support Dr. James Patrick Murphy and the Kentucky Society of Addiction Medicine by passing the ALARM Act, which repeal KY’s restrictive buprenorphine regulation 201 KAR 9:270.
Thanks! Now that you know my “ask,” please read on for the rest of the story…
IN RECORD NUMBERS, KENTUCKIANS CONTINUE TO DIE FROM OPIOIDS.
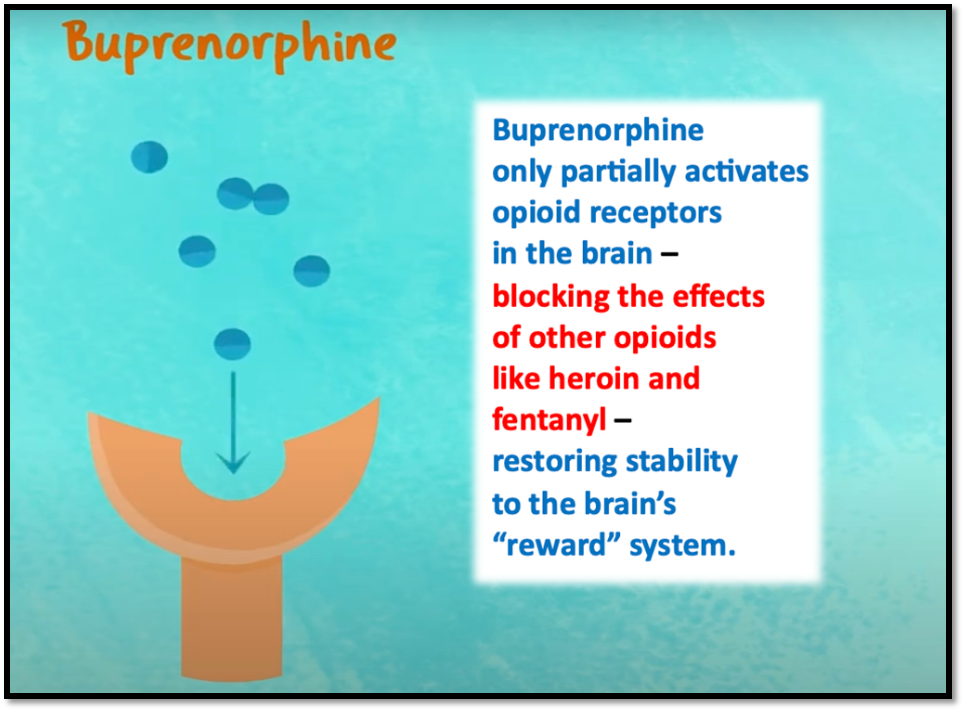
Widespread availability of buprenorphine could decrease overdose deaths by 50% or more. Buprenorphine (sometimes know by the trade name Suboxone) is FDA-approved to treat damaged areas in the brain that cause opioid addiction and can prevent dangerous addictive behaviors that lead to overdose.
Distinct from NARCAN – which might reverse an overdose but does not treat the actual addiction –buprenorphine treats the root cause of the overdose. Buprenorphine promotes recovery, reduces crime, prevents overdoses, and saves lives.
Buprenorphine treatment is not simply trading one drug dependency for another. Quite the opposite, buprenorphine is a prescription medicine that treats the disease process, allowing patients to lead productive heathy lives – in much the same way that insulin allows people with diabetes to manage their disease and live well.
Tragically, barriers to accessing buprenorphine exist, such as regulatory burdens, costs, stigma, and unfounded fear of diversion. Thus, only one in five Kentuckians who need buprenorphine can get treatment.
In Kentucky, a major barrier to buprenorphine treatment is 201 KAR 9:270 – an obsolete law that is not aligned with current clinical evidence. This onerous regulation restricts effective dosing and forces doctors and patients to complete costly, unnecessary tasks and imposes unscientific mandates that contradict recommendations of the overwhelming majority of experts. This is beyond illogical – it’s dangerous and deprives suffering people of lifesaving medication.
Ask yourself, would anyone be OK with treating breast cancer this way? Of course not. So why is Kentucky so restrictive with treating ADDICTION ? – the #1 cause of death for adults under the age of forty.
Kentucky is a an outlier. Our federal government and most other states have already done away with antiquated regulations like 201 KAR 9:270, allowing buprenorphine to be regulated like any other DEA schedule 3 controlled substance – as it should be. But Kentucky, despite ranking among the absolute worst states in terms of overdose deaths, somehow is still hanging on to 201 KAR 9:270. This must change. The regulation must be repealed.
The ALARM Act is a vital grass roots legislative initiative, supported by the Kentucky Society of Addiction Medicine and many others, that will repeal 201 KAR 9:270 and allow all Kentucky doctors to confidently treat their patients with buprenorphine – the “gold standard” medication for treating opioid addiction.
Every overdose death is PREVENTABLE.
Sound the ALARM !
Contact Your Kentucky legislators and ask them to support the ALARM Act.
(800) 372-7181 Monday-Friday 7am to 6pm
or
(502) 564-8100 Monday-Friday 8am to 4:30pm,
And email addresses can be found on their individual bio pages:
Buprenorphine is an FDA-approved medication for treating opioid use disorder, proven to be effective inpreventingoverdose deaths, reducing drug related crime, recidivism, and drug diversion, while saving valuable community resources.
However, Kentucky’s buprenorphine prescribing regulation 201 KAR 9:270 is outdated, unnecessary and harmful, because it creates barriers to accessing this lifesaving care.
Furthermore, despite all good intentions, this regulation paradoxically increases crime and diversion. Thus, for the safety of our communities, 201 KAR 9:270 must be repealed.
• Despite law enforcement, DEA, policy-makers, and medical experts universally calling for the removal of barriers to accessing buprenorphine, barriers continue to exist, e.g., stigma, costs, irrational fear of diversion, prescriber trepidation, and pharmacist and prescriber fear of regulatory scrutiny. 201 KAR 9:270 contributes to all of these barriers.
• 201 KAR 9:270 is a barrier to buprenorphine treatment, because it rigidly mandates actions that should be dependent on individual patient circumstances and prescriber clinical judgment; actions such as: frequent in-person evaluations, mandatory specialist consults, numerous urine drug tests, extensive labs, psychological counseling, outdated dosage limits, and irrational limits on medications for co-occurring conditions. Laws mandating such measures are not supported by scientific evidence, federal policies, or clinical practice guidelines from the American Society of Addiction Medicine.
• Frankly, Kentucky’s buprenorphine law 201 KAR 9:270 is years behind the times. To illustrate just how absurd it has become, consider that Kentucky requires a special DEA “X-Waiver” that doesn’t even exist anymore. On December 29, 2022, in an effort to increase access to buprenorphine, Congress eliminated all buprenorphine-specific federal regulations, e.g., the DEA “X-Waiver,” along with caps on the number of patients per prescriber, prescriber limits, mandated education. But 201 KAR 9:270 still requires prescribers to have the “X-Waiver.”
• In sum, Kentucky has perhaps the most outdated, draconian, and harmful buprenorphine regulation in our nation and is one of only 19 states that still have buprenorphine-specific regulations on their books. And sadly, prescriptions for buprenorphine in Kentucky have only decreased at a time when overdose rates are still at record levels. Repealing 201 KAR 9:270 is common sense.
Why is this so?
Because of rapidly evolving scientific and clinical knowledge, it’s impossible for policymakers to create regulations that strictly tell clinicians how to treat addiction with buprenorphine. Beyond that, Kentucky’s deliberate regulatory process is too slow and renders obsolete any attempt at reworking 201 KAR 9:270 even before the ink dries on the page.
Therefore, to save lives, reduce crime, and improve the health and well-being of our communities, please join the Kentucky Society of Addiction Medicine and support repeal of Kentucky’s buprenorphine regulation 201 KAR 9:270. This decade old law is outdated, unfixable, unnecessary, and harms the people it was intended to help. It mandates actions that are not supported by evidence, actions that inhibit access to treatment, actions that lead to increase drug related crime, and actions that promote fraud, waste, and abuse.
Rather than discourage drug diversion, 201 KAR 9:270 actually worsens drug related crime and diversion. And tragically, Kentuckians struggling with addiction are needlessly dying because of barriers to treatment caused by this law.
Repeal of 201 KAR 9:270 would allow buprenorphine to assume its rightful place in the category of DEA Schedule III medications with low risk, allowing clinicians to prescribe buprenorphine for its legitimate medical purpose in the usual course of sound professional practice. Make our communities safer and healthier. Repeal of 201 KAR 9:270 is critically necessary.
A summation of clinical, social, and scientific evidence, as well as expert opinion and federal policy focusing on DIVERSION, CRIME, and ACCESS:
Treatment with buprenorphine was associated with a REDUCTION IN ARRESTS, via Addiction Medicine, the official journal of ASAM. https://pubmed.ncbi.nlm.nih.gov/30916463/
Any steps taken to minimize buprenorphine DIVERSION and misuse must be careful not to undermine the positive patient and public health benefits gained from expanded treatment access, via University of Kentucky. https://pubmed.ncbi.nlm.nih.gov/25221984/
Barriers to treatment with buprenorphine include “Aggressive enforcement strategies by the DEA and several state attorneys general—including increases in raiding, auditing, and launching criminal investigations of waivered providers,” via National Academies of Science.https://nap.nationalacademies.org/read/25310/chapter/7#120
The Kentucky Medical Association (KMA), American Medical Association, and the American Society of Addiction Medicine (ASAM) support a bill (House Bill 121) that would remove insurance barriers to treatment with buprenorphine. The rationale supporting House Bill 121 (noted below) also supports the Kentucky Society of Addiction Medicine’s call for repeal of 201 KAR 9:270. For context, I encourage you to read the following “one-page” support document from the AMA:
For more information, please go to my blog CONFLUENTIAL TRUTH https://jamespmurphymd.com and start scrolling. Related stories begin with my post on June 28, 2024 about a petition to the Kentucky Board of Medical Licensure…
On September 20, 2024, NIDA Director, Dr. Nora Volkow, gave the keynote address at UofL’s Research!Louisville awards ceremony. Here’s some of what our nation’s top addiction researcher had to say…
The opioid crisis started more than two decades ago, and we have not solved it.
It has caused more people dying than COVID itself.
The people that have died from the opioid crisis, all of them could have been prevented. Every single one of them could have been prevented.
We know how to prevent an overdose.
Overdoses are happening throughout all of the ages, throughout the whole life span.
The rise in overdose crisis…they went up to 117,000 in one year, those numbers were driven predominantly by fentanyl.
We are seeing the decreases in fentanyl overdoses…the latest numbers are twelve percent (decrease).
Pain medications started the overdose crisis. It basically stabilized and it’s going down.
Similarly, heroin basically is accounting for a very very limited amount of overdoses. And this reflects the fact that the drug dealers actually don’t see any benefit for them, incentive for them, selling heroin. They sell fentanyl.
What has created the turn down of the curve (in overdoses)?
This is what’s likely to be accounting for it… In the field of opioid use disorder, which is different from actually any other field in the substance use disorders, we have extremely effective medications.
To start with, we have an incredible drug, naloxone. Naloxone is an opioid receptor antagonist.
When you give it (naloxone) to someone that overdoses, you reverse that overdose if they overdosed with an opioid…Whether it is fentanyl or heroin or an opioid medication, you need to give the naloxone, for it to be effective, rapidly and at the correct dose.
We are very lucky to have naloxone.
And then we have three different classes of medications, all targeting the opioid receptor system, but with different pharmacological effects, that are very effective in treating opioid use disorders.
Methadone…It has been in existence for, I think, sixty years.
Buprenorphine was approved at the beginning of the 2000s.
And then we have naltrexone, that was approved for opioid use disorder more recently.
Methadone – full agonist at the opioid receptor.
Buprenorphine – partial agonist.
These medications (methadone and buprenorphine) are effective in reducing drug taking, in reducing craving, in reducing withdrawal.
Except for naltrexone. Naltrexone does not, per se, reduce withdrawal, it reduces craving, and it improves mood.
They are very effective in preventing overdose.
So the challenge is, you say, if you have these medications that are being so effective, why are we having so many people dying of overdoses? And the answer is because we do have the medications, but they are not being given to those that need them.
Why are they not being used?
There are multiple issues.
A key one is the stigma and discrimination against addiction.
The healthcare system providers don’t want to treat people with a substance use disorder.
We have generated a specialized system for the treating of substance use disorders that is independent of the healthcare system. Which is a totally lost opportunity.
Across the continuum, how can we improve access to these medications for people that need them?
There’s no evidence, to my knowledge, that any of the harm reduction practices exacerbate or increase the rate of overdose. I don’t know of any evidence. On the other hand, there’s ample evidence to show that harm reduction practices significantly reduces mortality.
There was so much expectation that the removal of the (DEA) waiver would increase the number of practitioners prescribing buprenorphine, but it hasn’t happened. What the research has shown is that the number of prescribers giving buprenorphine has not increased very much…Restrictive practices don’t help…The issue to me, this is discrimination. There is discrimination also in the way that we set up the reimbursement of taking care of someone with a very complex and potentially fatal disease.
Thank you, Dr. Volkow. You knocked it out of the park!
And this statement by our NIDA Director bears repeating, because it is a call to action: “If you have these medication that are being so effective, why are we having so many people dying of overdoses? And the answer is because we do have the medications, but they are not being given to those that need them.“
On Monday 9/16/2024, under a brilliant baking sun, from the south lawn of the state Capitol, Governor Andy Beshear proclaimed September to be Recovery Month in Kentucky. To his left and to his right sat about twelve sun-drenched dignitaries, most wearing business attire meant for air-conditioned offices. As I stood there in the front row, myself baking in the sun, I realized two things early on: (1) I had made the right decision to come, and (2) my game time decision to wear my UofL Med School polo shirt instead of a coat and tie was the right move (Can you find me in the pic below?).
Screenshot
I’d never heard Governor Beshear speak in person, and I found him to be as charming, personable, likable, and relatable as he always appears to be on TV. The governor said all the right things that needed to be said. He was inspirational as he recounted the work that had been done by Kentucky’s government over the past year battling the opioid crisis in our state. He touted KY’s 9.8% drop in overdose deaths from a year ago. He also said “There is a lot of work left to do.”
Eric Friedlander, Secretary of KY’s Cabinet for Health and Family Services also spoke and said he is thankful he is working for a Governor who “believes in science.”
And Lisa Lee, Commissioner for the Dept. for Medicaid, said that we’ve made progress, but she won’t be satisfied “until all barriers to treatment are gone.”
Others eloquently spoke, bills were ceremoniously signed, a few people with lived experience offered their compelling stories to the crowd, which dwindled a bit over time as onlookers gradually receded into the few shady spots farther away from the podium. All in all, the message was very positive. And as I stood in the front row to the right of the stage, facing Representative Kim Moser, the only other person besides me wearing red in Frankfort that day, I really wanted to believe the Governor when he said in closing, “I am convinced that we can defeat this epidemic.”
After the speeches, Representative Moser visited with me, offered me some of her views, gave me a little advice, and graciously invited me to come back to Frankfort in October to testify before her colleagues. She also introduced me to Secretary Friedlander, who I chatted with briefly. And before I left the podium area I got to speak with a true KY hero, Van Ingram, Executive Director for the Kentucky Office of Drug Control Policy.
These were all great connections to make. I had travelled to Frankfort thinking my main objective was to meet some of the people who I’ve been emailing regularly about the urgent need for a major overhaul of KY’s outdated and harmful regulation governing how physicians prescribe buprenorphine to treat addiction. I felt that my meet-and-greet mission had been accomplished. I could now report back to my organizations (i.e., KYSAM, ASAM, AMA, KYHRC) that our concerns about the buprenorphine regulation were probably a little closer to getting heard by the people who could bring about the needed change.
What happened next was unexpected.
I walked to the far end of the road between the Capitol and the Annex Building where dozens of addiction treatment, addiction recovery, and addiction support groups had set up tents, tables, and booths. I decided to visit every group represented there. I learned what they did, how they were funded, what role they played in the orchestra of helpers throughout our state. I met some amazing people, and I am definitely going to follow up with as many as I can. We truly have some fantastic advocates and caregivers in our state.
And maybe providence had a plan for me that day, because as I worked my way along that road from the far end to the beginning, near the humongous, beautiful, and famous floral clock on the Capitol grounds, the last group I visited was comprised of only two women. Out of respect for their privacy, I won’t go into specifics. But suffice it to say, these two amazing individuals were living fulfilling lives in recovery from opioid addiction, both were being treated with buprenorphine, and both told me that treatment with buprenorphine had literally saved each of their lives.
With this as my send off, I left the Capitol a little more sunburned but tremendously more inspired. It’s clear, there are a lot of wonderful people in our state doing fantastic things to help people with addiction make it to their promised land of recovery. And I’m more determined than ever to prove myself worthy of inclusion amongst the ranks of these dedicated and compassionate healers, by virtue of my doctoring, my advocacy, and my caring.
If you’ve read all the way down to this point in my article, then you are likely one of those wonderful people I mentioned in the paragraph above – because I know my writing is nowhere near as compelling as the cause. And you’re probably a person who wants to make a difference – maybe even save a life in the process. If so, then I have an ask of you…
Please help me get the message to our Governor that Kentucky’s outdated buprenorphine regulation needs to be gone. The science, the data, and the lived experience of thousands in recovery confirm that buprenorphine treatment for opioid addiction promotes recovery, prevents overdoses, and saves lives. I made some handouts that I gave to people at the Recovery Month event on the Capitol lawn. Below you will find screen shots of the handouts.
As I said to one nice young lady, who politely told me that because she was employed by the state there was no way she could advocate for changing a state regulation, “That’s all right. I’m just asking that you read it.”
“Why?” she asked.
“Because, once you read it, you can’t un-read it.”
So, now I humbly ask you to please read the information below. And if you want to help remove a significant barrier to people with addiction receiving the most effective treatment we have to prevent overdoses and promote recovery, then stoke your creativity, ingenuity, determination, and problem-solving skills and help me find a way to get this information to Governor Beshear.
As Secretary Friedlander said, our Governor believes science.
Then you will know the truth, and the truth will set you free. ~ John 8:32 (NIV)
…Pain free?
Confluential Truth blog posts address various issues, and many share a healthcare theme. Often the focus is on chronic pain. The following collection of Confluential Truth offers my views on how chronic pain may be effectively and safely treated, especially when the treatment involves controlled substances. Each essay is like a chapter in a mini-textbook about treating chronic pain. They are offered here hoping to provide insight into improving quality of life for pain sufferers and pain care providers.
*
PROLOGUE: The Algiatrist – To set the tone, a poem about treating pain and being “useful.”
CHAPTER ONE: The Dream of Pain Care – A transcript of my address to the physicians and staff of Norton Healthcare – the what, why & how. If you only have time to read one essay, this is the one.
CHAPTER FIVE: Treating Pain Patients Like Addicts – There is ample overlap between optimal treatment for addiction and optimal treatment for chronic pain. Utilizing this knowledge can enhance the effectiveness and mitigate the risks inherent to treating chronic pain with controlled substances.https://jamespmurphymd.com/2014/11/21/treating-pain-patients-like-addicts
*
CHAPTER SIX: Basic Pain Care Certification – It’s a sad fact the number of deaths associated with drug overdose is roughly equivalent to the number of motor vehicle fatalities. Imagine how many might die on our roads if, instead of a driver’s license, all you needed to drive a car was a prescription from a doctor. Now, imagine how many less might die of drug overdose if you had earn a “license” to use controlled substances…
CHAPTER SEVEN: Strength in Numbers – Successful chronic pain treatment involves: (a) medical care; (b) counseling; and (c) a support system. Find all three and you have probably found…
CHAPTER EIGHT: It’s Only Words – Over the years I have given many presentations concerning medication management for chronic pain. Often I have said that if there is only one concept I want the group to take away it’s that “addiction” and “physical dependence” are not the same thing.
CHAPTER NINE: Talking Trash – We spend much time worrying about the acquisition of pain medications but too often don’t know what to do with them when we are done.
James Patrick Murphy, MD, MMM is Chair of the Board of Governors -and Immediate Past President- of the Greater Louisville Medical Society, Medical Director of Murphy Pain Center, and an Assistant Clinical Professor at the University of Louisville School of Medicine. Dr. Murphy contributes to numerous publications, has presented before national and international audiences, and consults with a wide spectrum of agencies and individuals regarding pain, addiction, and the future of healthcare in our country. He is board-certified in Pain Medicine, Anesthesiology, and Addiction Medicine.
THE CHRONIC PAIN PATIENT’S GUIDE TO INDIANA’S REGULATIONS
No man is an island, Entire of itself, Every man is a piece of the continent, A part of the main. – John Donne
The poet, John Donne, knew it. Every Hoosier pain patient and Hoosier pain care provider should take it to heart. No patient or provider is an island. And pain care is best when there is a partnership between the patient and provider. The Pathway to Partnership If you are treated for pain in the Hoosier State the pathway to partnership with your physician passes through Indiana’s pain regulations. Indiana’s entire southern border is Kentucky. And when it comes to patient responsibilities, Kentucky’s pain regulations have much in common with Indiana’s. Therefore, Hoosier patients can begin preparation for their Indiana chronic pain care evaluation by reading my article: Pathway to Partnership, Part I (KY) – The Chronic Pain Patient’s Guide to Kentucky’s Regulations.Available at: https://jamespmurphymd.com/2015/02/13/pathway-to-partnership Particular to Indiana is the Hoosier state’s emphasis on medication dosing limits that trigger mandatory compliance with the regulations. Calculating these dosing limits can be quite confusing and, frankly, patients are not responsible for knowing them. Prescribers are. But to be a good “partner” with your prescriber, you should at least become familiar with these dosing limits. Later in this article I will summarize. But first, in order to hold up your end of the partnership, here are ten items you can prepare:
Insider Information As a partner, you are entitled to some “insider” information. Here it is… A new section of Indiana’s regulations contain a lengthy explanation of what prescribers must consider when ordering drug screens. By doing so, this section offers insight into appropriate patient behavior. The following list, summarized from the regulations, offers an insider’s look at what Indiana expects of a pain patient: “In determining whether a drug monitoring test…is medically necessary, the physician shall consider” if the patient has:
Refused or failed to follow through with exams/tests?
Just not done well overall?
Bottom line: Be honest, up front and “transparent.” No one likes surprises. A good partnership is all about trust and communication. Understand what your treatment agreement says and live up to it. Dosing Limits Now, about those dosing limits… As I said, it can be confusing, but you should try to understand the concepts and discuss them with your prescriber. Not all pain prescriptions are subject to the Indiana regulations. Therefore, it is important to understand the dosing limits that trigger mandatory compliance. These limits are dependent upon: (1) the dose, (2) the quantity and (3) the duration. The Morphine Equivalent Dose (“MED”) is basically how strong your medication would be if it were to be substituted for morphine. This is very important to INDIANA regulatory agencies. I highly recommend you learn how to calculate your MED. Calculating the MEDStep ONE: Calculate the MED for one pill Determine the dose of morphine that would be equal to one of your pills using a standard conversion table (For example: a FIVE mgm hydrocodone pill is the same as a FIVE mgm morphine pill; but a FIVE mgm oxycodone pill would be the same as a 7.5 mgm morphine pill). Indiana officials recommend this website for help with making this determination: The online opioid calculator from GlobalRPHhttp://www.globalrph.com/narcoticonv.htmStep TWO: Calculate your DAILY MED Once you have converted your pill to its “morphine equivalent,” simply add up the maximum number of pills your prescription allows you to take in a day and multiply this number by the morphine equivalent (MED) you determined in step one. (Number of pills per day) x MED/one pill = Daily MED For example: Since a FIVE mgm hydrocodone pill is equal to a FIVE mgm morphine pill, the daily MED of someone taking THREE of these hydrocodone pills per day would be: 5 mgm x 3 pills per day = 15 mgm MED Here are some common ORALLY prescribed opioids that compare to a MED of 15: Hydrocodone (oral) 15 mgm/day = 15 mgm of morphine (oral) Oxycodone(oral) 10 mgm/day = 15 mgm of morphine (oral) Oxymorphone (oral) 5 mgm/day = 15 mgm of morphine (oral)Codeine (oral) mgm/day = 15 mgm of morphine (oral)Hydromorphone (oral) 3.75 mgm/day = 15 mgm of morphine (oral)Tramadol (oral) 150 = 15 mgm of morphine (oral)Note: MED greater than SIXTY If you are on a treatment regimen with a morphine equivalent dose of more than SIXTY (60) MED, the physician may require you to have an evaluation by a specialist. According to the regulations, your physician must explain to you that there is an increased risk of adverse outcomes, including death, when your daily MED is greater than SIXTY. So now that you understand the MED, you are ready to look at the DOSING LIMITS that trigger compliance with the regulations. DOSE, QUANTITY & DURATION When any of the following conditions are met, your physician (and you) must comply with the Indiana pain regulations.
DOSE & DURATION >15 MED for >3 months
DAILY MED greater than FIFTEEN for DURATION of more than three consecutive months Or…
QUANTITY & DURATION >60 pills for >3 months
More than SIXTY opioid pills per month for DURATION of more than THREE consecutive months Or…
PATCHES > 3 months
Any opioid skin patches (e.g., fentanyl or buprenorphine), regardless of the dose or quantity, for DURATION of more than THREE consecutive months Or…
Hydrocodone-Only Extended Release
Any hydrocodone-only extended release medication that is NOT in an “abuse deterrent” form, regardless of the DOSE, QUANTITY or DURATION Or…
TRAMADOL (My advice) >150 mgm for >3 months
Actual language in the regulations state: “If the patient’s tramadol dose reaches a morphine equivalent dose of more than sixty (60) milligrams per day for more than three (3) consecutive months.” This tramadol dose limit seems to be overly generous when compared to other MED dosing limits. A SIXTY (60) MGM MED of tramadol is in the range of 300 to 600 mgm of tramadol. Considering that the maximum therapeutic dose for tramadol is only400 mgm per day, one could potentially exceed the safe upper limit of tramadol and still not exceed Indiana’s dosing limit. This seems to be inconsistent with the regulation’s other opioid dosing limits. My advice: Since 150 mgm of tramadol is equivalent to a FIFTEEN (15) MED, I believe it is more consistent with the other Indiana opioid dosage limits to consider TRAMADOL greater than 150 mgm/day for more than THREE consecutive months as the dosage limit congruent with other opioid dosage limits. Reference: The online opioid calculator from GlobalRPH http://www.globalrph.com/narcoticonv.htmWait!!! There are EXEMPTIONS !!! Regardless of the dose, quantity or duration, the Indiana pain regulations do not apply to these patients: (1) With a terminal condition (2) Residing in a licensed health facility (3) Enrolled in a licensed hospice program (4) Enrolled in a licensed palliative care program In summary, patients and physicians should travel the pathway to partnership together. Patients can do their part by (1) preparing for the clinical visits, (2) understanding and adhering to their treatment agreements, and (3) educating themselves about risks, side-effects, and legal aspects of their care. It is a real challenge to treat chronic pain in this day and age. Your physician needs your help. Will you leave it all up to your physician? Or will you be a good partner, heeding the words of the poet Donne… And therefore never send to knowFor whom the bell tolls;It tolls for thee. *James Patrick Murphy, MD, MMM is Chair of the Board of Governors -and Immediate Past President- of the Greater Louisville Medical Society, Medical Director of Murphy Pain Center, and an Assistant Clinical Professor at the University of Louisville School of Medicine. Dr. Murphy contributes to numerous publications, has presented before national and international audiences, and consults with a wide spectrum of agencies and individuals regarding pain, addiction, and the future of healthcare in our country. He is board-certified in Pain Medicine, Anesthesiology, and Addiction Medicine. * References and links pertaining to this article are provided in the comments. * This unofficial summary is my personal opinion. A full, official version of the final rule should be consulted for compliance purposes at: http://www.in.gov/legislative/iac/20141105-IR-844140289FRA.xml.html The Indian State Medical Association also has a summary available at: http://www.ismanet.org/pdf/legal/IndianaPainManagementPrescribingFinalRuleSummary.pdf And if you really want to explore the Indiana pain regulations in detail, there is no better source than the online guide: First Do No Harm, The Indiana Healthcare Providers Guide to the Safe, Effective Management of Chronic Non-Terminal Pain.http://www.in.gov/bitterpill/docs/First_Do_No_Harm_V_1_0.pdf * Hey Hoosier! Who’s your partner? * * *

















 https://jamespmurphymd.com/2014/03/18/is-there-method-to-this-march-madness
https://jamespmurphymd.com/2014/03/18/is-there-method-to-this-march-madness