 Kentucky’s controlled substances regulations make clear distinctions between: (1) initial prescribing, (2) prescribing by the three-month mark, and (3) prescribing beyond three months. To make matters even more confusing, the regulations are two-tiered, with specific language pertaining only to schedule II drugs, with schedule V drugs being exempt from the regulations.
Kentucky’s controlled substances regulations make clear distinctions between: (1) initial prescribing, (2) prescribing by the three-month mark, and (3) prescribing beyond three months. To make matters even more confusing, the regulations are two-tiered, with specific language pertaining only to schedule II drugs, with schedule V drugs being exempt from the regulations.
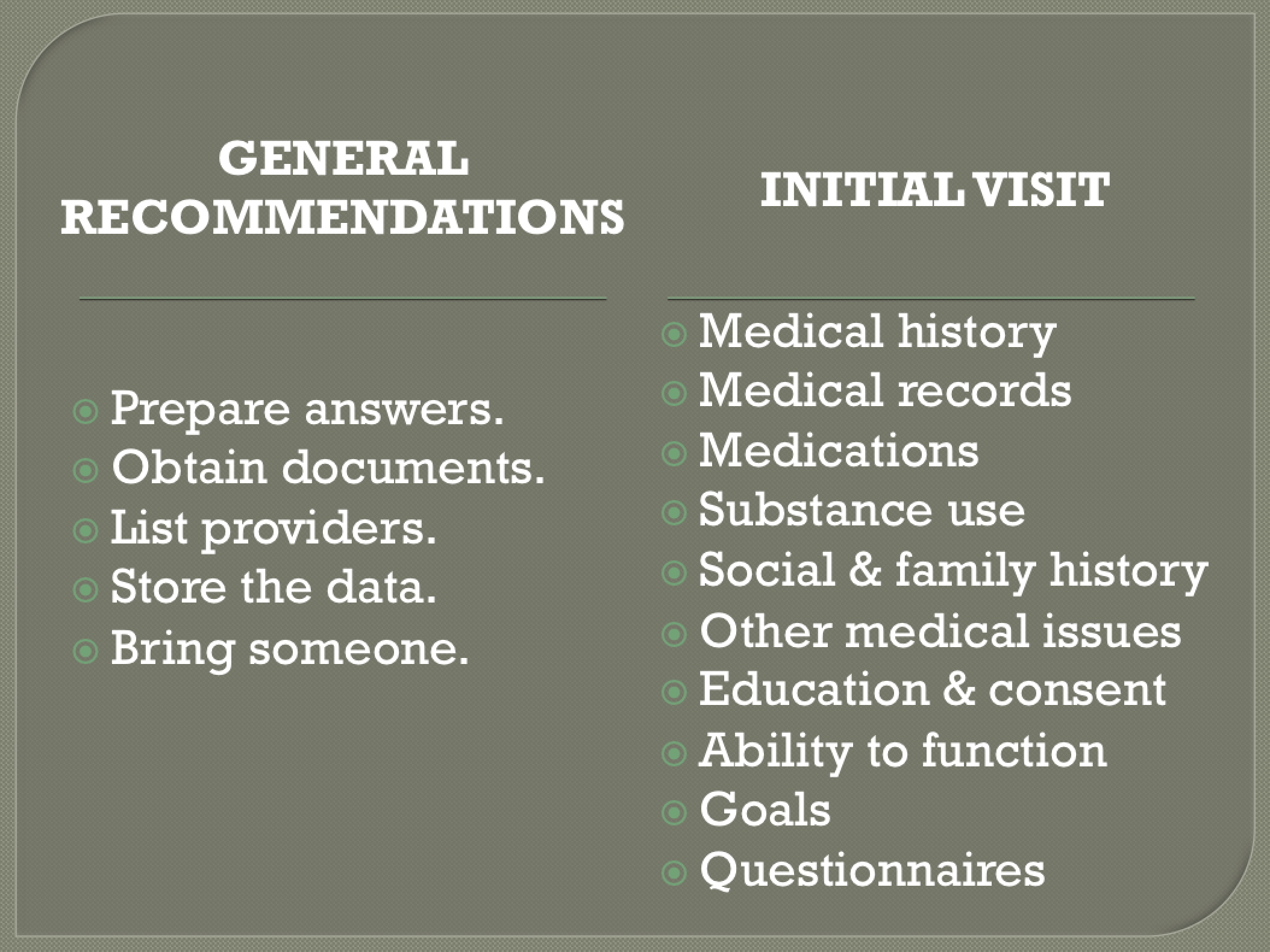
Because of some seemingly redundant and contradictory language, understanding Kentucky’s regulations can be challenging. Prescriber uncertainty can interfere with proper patient care. In an effort to simplify this process I have summarized Kentucky’s regulations governing the initial prescribing of controlled substances in a convenient “check list” format. Future articles will look at the three-month mark and beyond.

The bold components of the checklist are required only when prescribing schedule II controlled substances. However, to be safe I recommend checking off all of the requirements when prescribing any schedule II-IV drug.
Note: I am a physician; not a lawyer. This summary is not legal advice. Each facility and physician should consult its own legal counsel for advice and guidance.

P lan to T H I N K
What to do initially when prescribing during the first three months of treatment.
P lan
___ Deliberate decision that it is medically appropriate to prescribe or dispense the controlled substance in the amount specified
___ Written plan stating the objectives of the treatment
____Written plan stating any further diagnostic examinations
T each
___ Safe use
___ A controlled substance for an acute complaint is for time-limited use
___ Discontinue medication when the condition has resolved
___ Proper disposal of any unused medications
___ KBML website resources
Note: Educational materials relating to these subjects may be found on the board’s web site, www.kbml.ky.gov or
http://kbml.ky.gov/hb1/Pages/Considerations-For-Patient-Education.aspx
H istory and physical
___ Appropriate medical history relevant to the medical complaint, including a history of present illness
___ Physical examination of the patient relevant to the medical complaint and related symptoms
I nformed consent
__ Discuss the benefits and risks of prescribing or dispensing a controlled substance to the patient, including:
(a) nontreatment, (b) other treatment, (c) the risk of tolerance and (d) the risk of drug dependence
__ Obtain written consent for the treatment.
N o long-acting opioids
___ No long-acting or controlled-release opioids for acute pain that is not directly related to and “close in time” to a specific surgical procedure
K ASPER
___ Obtain and review KASPER report for that patient for the preceding 12 months
___ Appropriately utilize KASPER information in evaluation and treatment
Additional documentation required for patient prescribed a schedule II controlled substance, as “appropriate”:
___Diagnostics (labs, studies, etc.)
___Evaluations and consultations;
___Treatments and outcomes
___Medications (date, type, dosage, and quantity)
___Instructions
___Agreements
When prescribing “additional” Schedule II, at “reasonable” and individualized intervals review:
___ Plan of care
___ Provide any new information about the treatment
___ Modify or terminate the treatment as appropriate
EXEMPTIONS to Kentucky’s regulations:
The exemptions are very confusing. While the first set of exemptions (see below) are supposed to apply to all controlled substance, there are additional exemptions that pertain only to schedule II controlled substances.
I believe the most important points here are:
- Cancer patients are exempted.
- In-patients are exempted for Schedule III-IV
- In-patients receiving schedule II drugs must have a KASPER, but all the treating physicians can share the report.
- Post-op schedule II drugs are exempted for 2 weeks.
- Schedule V drugs are always exempted.
Here are the exemptions in detail:
Kentucky’s regulations shall not apply to a physician prescribing or dispensing a controlled substance:
(a) To a patient as part of the patient’s hospice or end-of-life treatment;
(b) To a patient admitted to a licensed hospital as an inpatient, outpatient, or observation patient, during and as part of a normal and expected part of the patient’s course of care at that hospital;
(c) To a patient for the treatment of pain associated with cancer or with the treatment of cancer;
(d) To a patient who is a registered resident of a long-term-care facility as defined in KRS 216.510;
(e) During the effective period of any period of disaster or mass casualties which has a direct impact upon the physician’s practice;
(f) In a single dose prescribed or dispensed to relieve the anxiety, pain, or discomfort experienced by that patient submitting to a diagnostic test or procedure; or
(g) That has been classified as a Schedule V controlled substance.
But wait! There are more exemptions that pertain only when prescribing Schedule II controlled substances…
For each patient for whom a physician prescribes or dispenses a Schedule II these regulations shall not apply to:
- A physician prescribing or administering that controlled substance immediately prior to, during, or within the fourteen (14) days following an operative or invasive procedure or a delivery if the prescribing or administering is medically related to the operative or invasive procedure or delivery and the medication usage does not extend beyond the fourteen (14) days; or
- For administration in a hospital or long-term-care facility if the hospital or long-term-care facility with an institutional account, or a physician in those hospitals or facilities if no institutional account exists, queries KASPER for all available data on the patient or resident for the twelve (12) month period immediately preceding the query, within twelve (12) hours of the patient’s or resident’s admission, and places a copy of the query in the patient’s or resident’s medical records for use during the duration of the patient’s stay at the facility;
- As part of the patient’s hospice or end-of-life treatment;
- For the treatment of pain associated with cancer or with the treatment of cancer;
- In a single dose to relieve the anxiety, pain, or discomfort experienced by a patient submitting to a diagnostic test or procedure;
- Within seven (7) days of an initial prescribing or dispensing under subsection (1) of this section if the prescribing or dispensing:
- Is done as a substitute for the initial prescribing or dispensing;
- Cancels any refills for the initial prescription; and
- Requires the patient to dispose of any remaining unconsumed medication;
- Within ninety (90) days of an initial prescribing or dispensing under subsection (1) of this section if the prescribing or dispensing is done by another physician in the same practice or in an existing coverage arrangement, if done for the same patient for the same medical condition; or
- To a research subject enrolled in a research protocol approved by an institutional review board that has an active federalwide assurance number from the United States Department for Health and Human Services, Office for Human Research Protections if the research involves single, double, or triple blind drug administration or is additionally covered by a certificate of confidentiality from the National Institutes of Health.
There are additional “Professional Standards for Commencing Long Term Use of Prescribing or Dispensing of Controlled Substances for the Treatment of Pain and Related Symptoms Associated with a Primary Medical Complaint” that must be met before a physician commences to prescribe or dispense any controlled substance to a patient sixteen (16) years or older for pain or other symptoms associated with the same primary medical complaint for a total period of longer than three (3) months.
To address this information and much more, there will be another Confluential Truth article coming soon. You may also refer to the regulations as posted on the KBML website (http://kbml.ky.gov/hb1/Pages/House-Bill-1-Ordinary-Regulations.aspx) and in the “comments” section accompanying this article.

***
**
*








 https://jamespmurphymd.com/2014/03/18/is-there-method-to-this-march-madness
https://jamespmurphymd.com/2014/03/18/is-there-method-to-this-march-madness