THE CHRONIC PAIN PATIENT’S GUIDE TO INDIANA’S REGULATIONS 
No man is an island, Entire of itself, Every man is a piece of the continent, A part of the main. – John Donne
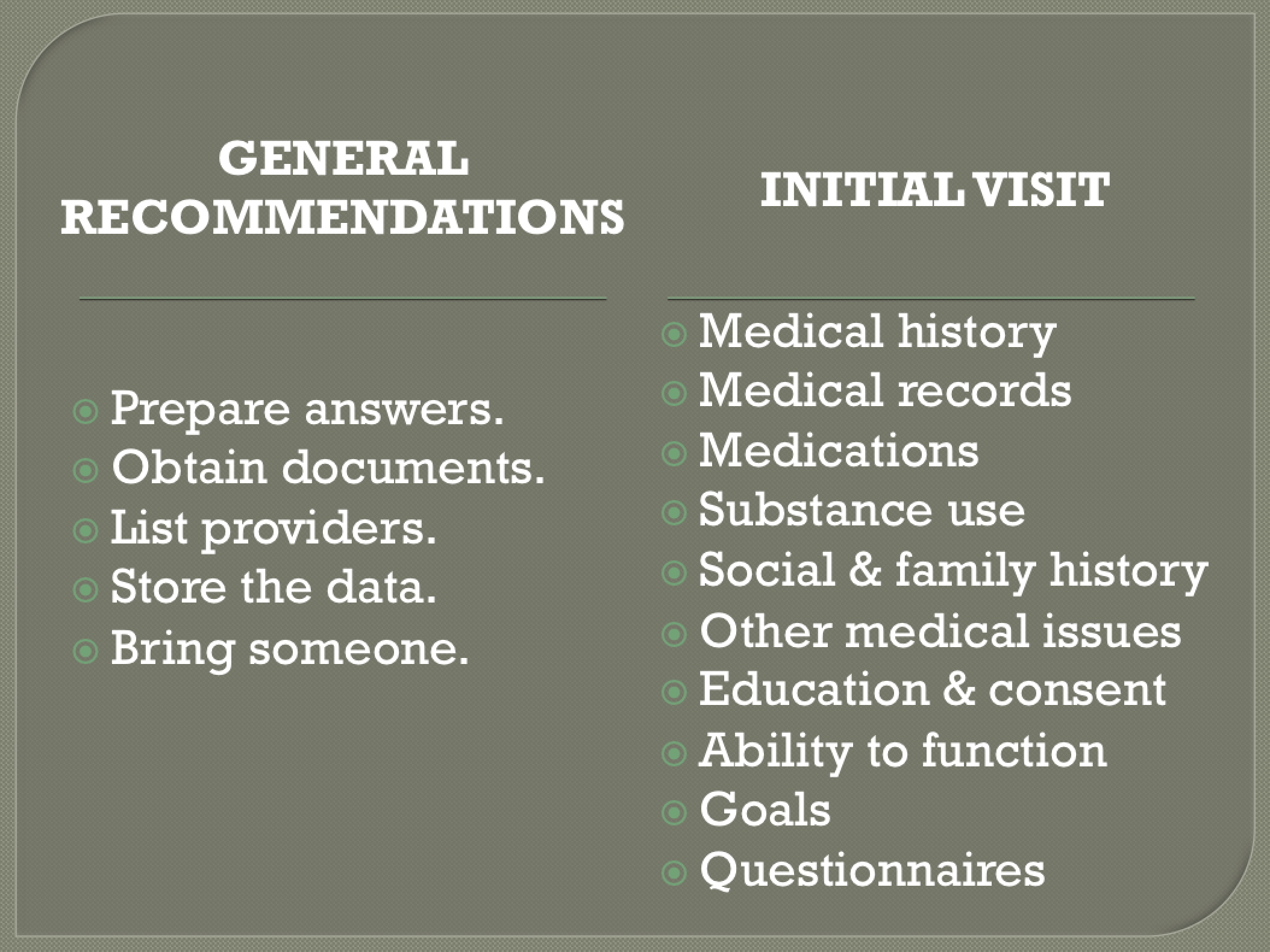
The poet, John Donne, knew it. Every Hoosier pain patient and Hoosier pain care provider should take it to heart. No patient or provider is an island. And pain care is best when there is a partnership between the patient and provider. The Pathway to Partnership If you are treated for pain in the Hoosier State the pathway to partnership with your physician passes through Indiana’s pain regulations. Indiana’s entire southern border is Kentucky. And when it comes to patient responsibilities, Kentucky’s pain regulations have much in common with Indiana’s. Therefore, Hoosier patients can begin preparation for their Indiana chronic pain care evaluation by reading my article: Pathway to Partnership, Part I (KY) – The Chronic Pain Patient’s Guide to Kentucky’s Regulations.  Available at: https://jamespmurphymd.com/2015/02/13/pathway-to-partnership Particular to Indiana is the Hoosier state’s emphasis on medication dosing limits that trigger mandatory compliance with the regulations. Calculating these dosing limits can be quite confusing and, frankly, patients are not responsible for knowing them. Prescribers are. But to be a good “partner” with your prescriber, you should at least become familiar with these dosing limits. Later in this article I will summarize. But first, in order to hold up your end of the partnership, here are ten items you can prepare:
Available at: https://jamespmurphymd.com/2015/02/13/pathway-to-partnership Particular to Indiana is the Hoosier state’s emphasis on medication dosing limits that trigger mandatory compliance with the regulations. Calculating these dosing limits can be quite confusing and, frankly, patients are not responsible for knowing them. Prescribers are. But to be a good “partner” with your prescriber, you should at least become familiar with these dosing limits. Later in this article I will summarize. But first, in order to hold up your end of the partnership, here are ten items you can prepare:
- Your past medical history
- Your pertinent medical records
- An accurate medication list
- Any substance abuse history
- Your social and family history
- Any other medical issues
- Educate yourself for proper informed consent
- Your current level of function
- Your treatment goals
- Complete questionnaires & mental health screens
These ten items are discussed in detail in Pathway to Partnership, Part I (KY) – The Chronic Pain Patient’s Guide to Kentucky’s Regulations. Prepare as described above you will be well on your way to becoming a great partner in your care. As your partnership continues, expect to have contact with your physician on a regular basis and even randomly to:
- Review your progress with your treatment plan;
- Review the goals of your plan; and
- Review expectations (i.e. attending therapy, counseling, tests, etc.)
Insider Information As a partner, you are entitled to some “insider” information. Here it is… A new section of Indiana’s regulations contain a lengthy explanation of what prescribers must consider when ordering drug screens. By doing so, this section offers insight into appropriate patient behavior. The following list, summarized from the regulations, offers an insider’s look at what Indiana expects of a pain patient: “In determining whether a drug monitoring test…is medically necessary, the physician shall consider” if the patient has:
- Taken the meds as prescribed?
- Taken more meds than allowed?
- Given or sold meds to anyone?
- Benefitted from the meds?
- Taken any other drugs – legal or illegal?
- Been honest and up front about past drug use?
- Tried to get early refills?
- Lost meds? Had them stolen?
- Had an abnormal INSPECT state prescription report?
- Failed a drug screen?
- Been intoxicated?
- Been acting aggressive, depressed, anxious, etc.?
- Been diagnosed with a psychiatric condition?
- Demanded certain specific meds?
- Had a major illness? Pregnancy? Hospitalization?
- Been resistant to any changes in the care plan?
- Refused or failed to follow through with exams/tests?
- Just not done well overall?
Bottom line: Be honest, up front and “transparent.” No one likes surprises. A good partnership is all about trust and communication. Understand what your treatment agreement says and live up to it.  Dosing Limits Now, about those dosing limits… As I said, it can be confusing, but you should try to understand the concepts and discuss them with your prescriber. Not all pain prescriptions are subject to the Indiana regulations. Therefore, it is important to understand the dosing limits that trigger mandatory compliance. These limits are dependent upon: (1) the dose, (2) the quantity and (3) the duration. The Morphine Equivalent Dose (“MED”) is basically how strong your medication would be if it were to be substituted for morphine. This is very important to INDIANA regulatory agencies. I highly recommend you learn how to calculate your MED.
Dosing Limits Now, about those dosing limits… As I said, it can be confusing, but you should try to understand the concepts and discuss them with your prescriber. Not all pain prescriptions are subject to the Indiana regulations. Therefore, it is important to understand the dosing limits that trigger mandatory compliance. These limits are dependent upon: (1) the dose, (2) the quantity and (3) the duration. The Morphine Equivalent Dose (“MED”) is basically how strong your medication would be if it were to be substituted for morphine. This is very important to INDIANA regulatory agencies. I highly recommend you learn how to calculate your MED.  Calculating the MED Step ONE: Calculate the MED for one pill Determine the dose of morphine that would be equal to one of your pills using a standard conversion table (For example: a FIVE mgm hydrocodone pill is the same as a FIVE mgm morphine pill; but a FIVE mgm oxycodone pill would be the same as a 7.5 mgm morphine pill). Indiana officials recommend this website for help with making this determination: The online opioid calculator from GlobalRPH http://www.globalrph.com/narcoticonv.htm
Calculating the MED Step ONE: Calculate the MED for one pill Determine the dose of morphine that would be equal to one of your pills using a standard conversion table (For example: a FIVE mgm hydrocodone pill is the same as a FIVE mgm morphine pill; but a FIVE mgm oxycodone pill would be the same as a 7.5 mgm morphine pill). Indiana officials recommend this website for help with making this determination: The online opioid calculator from GlobalRPH http://www.globalrph.com/narcoticonv.htm  Step TWO: Calculate your DAILY MED Once you have converted your pill to its “morphine equivalent,” simply add up the maximum number of pills your prescription allows you to take in a day and multiply this number by the morphine equivalent (MED) you determined in step one. (Number of pills per day) x MED/one pill = Daily MED For example: Since a FIVE mgm hydrocodone pill is equal to a FIVE mgm morphine pill, the daily MED of someone taking THREE of these hydrocodone pills per day would be: 5 mgm x 3 pills per day = 15 mgm MED Here are some common ORALLY prescribed opioids that compare to a MED of 15: Hydrocodone (oral) 15 mgm/day = 15 mgm of morphine (oral) Oxycodone(oral) 10 mgm/day = 15 mgm of morphine (oral) Oxymorphone (oral) 5 mgm/day = 15 mgm of morphine (oral) Codeine (oral) mgm/day = 15 mgm of morphine (oral) Hydromorphone (oral) 3.75 mgm/day = 15 mgm of morphine (oral) Tramadol (oral) 150 = 15 mgm of morphine (oral) Note: MED greater than SIXTY If you are on a treatment regimen with a morphine equivalent dose of more than SIXTY (60) MED, the physician may require you to have an evaluation by a specialist. According to the regulations, your physician must explain to you that there is an increased risk of adverse outcomes, including death, when your daily MED is greater than SIXTY. So now that you understand the MED, you are ready to look at the DOSING LIMITS that trigger compliance with the regulations. DOSE, QUANTITY & DURATION When any of the following conditions are met, your physician (and you) must comply with the Indiana pain regulations.
Step TWO: Calculate your DAILY MED Once you have converted your pill to its “morphine equivalent,” simply add up the maximum number of pills your prescription allows you to take in a day and multiply this number by the morphine equivalent (MED) you determined in step one. (Number of pills per day) x MED/one pill = Daily MED For example: Since a FIVE mgm hydrocodone pill is equal to a FIVE mgm morphine pill, the daily MED of someone taking THREE of these hydrocodone pills per day would be: 5 mgm x 3 pills per day = 15 mgm MED Here are some common ORALLY prescribed opioids that compare to a MED of 15: Hydrocodone (oral) 15 mgm/day = 15 mgm of morphine (oral) Oxycodone(oral) 10 mgm/day = 15 mgm of morphine (oral) Oxymorphone (oral) 5 mgm/day = 15 mgm of morphine (oral) Codeine (oral) mgm/day = 15 mgm of morphine (oral) Hydromorphone (oral) 3.75 mgm/day = 15 mgm of morphine (oral) Tramadol (oral) 150 = 15 mgm of morphine (oral) Note: MED greater than SIXTY If you are on a treatment regimen with a morphine equivalent dose of more than SIXTY (60) MED, the physician may require you to have an evaluation by a specialist. According to the regulations, your physician must explain to you that there is an increased risk of adverse outcomes, including death, when your daily MED is greater than SIXTY. So now that you understand the MED, you are ready to look at the DOSING LIMITS that trigger compliance with the regulations. DOSE, QUANTITY & DURATION When any of the following conditions are met, your physician (and you) must comply with the Indiana pain regulations.
- DOSE & DURATION >15 MED for >3 months
DAILY MED greater than FIFTEEN for DURATION of more than three consecutive months Or…
- QUANTITY & DURATION >60 pills for >3 months
More than SIXTY opioid pills per month for DURATION of more than THREE consecutive months Or…
- PATCHES > 3 months
Any opioid skin patches (e.g., fentanyl or buprenorphine), regardless of the dose or quantity, for DURATION of more than THREE consecutive months Or…
- Hydrocodone-Only Extended Release
Any hydrocodone-only extended release medication that is NOT in an “abuse deterrent” form, regardless of the DOSE, QUANTITY or DURATION Or…
- TRAMADOL (My advice) >150 mgm for >3 months
Actual language in the regulations state: “If the patient’s tramadol dose reaches a morphine equivalent dose of more than sixty (60) milligrams per day for more than three (3) consecutive months.” This tramadol dose limit seems to be overly generous when compared to other MED dosing limits. A SIXTY (60) MGM MED of tramadol is in the range of 300 to 600 mgm of tramadol. Considering that the maximum therapeutic dose for tramadol is only 400 mgm per day, one could potentially exceed the safe upper limit of tramadol and still not exceed Indiana’s dosing limit. This seems to be inconsistent with the regulation’s other opioid dosing limits. My advice: Since 150 mgm of tramadol is equivalent to a FIFTEEN (15) MED, I believe it is more consistent with the other Indiana opioid dosage limits to consider TRAMADOL greater than 150 mgm/day for more than THREE consecutive months as the dosage limit congruent with other opioid dosage limits. Reference: The online opioid calculator from GlobalRPH http://www.globalrph.com/narcoticonv.htm Wait!!! There are EXEMPTIONS !!! Regardless of the dose, quantity or duration, the Indiana pain regulations do not apply to these patients: (1) With a terminal condition (2) Residing in a licensed health facility (3) Enrolled in a licensed hospice program (4) Enrolled in a licensed palliative care program  In summary, patients and physicians should travel the pathway to partnership together. Patients can do their part by (1) preparing for the clinical visits, (2) understanding and adhering to their treatment agreements, and (3) educating themselves about risks, side-effects, and legal aspects of their care. It is a real challenge to treat chronic pain in this day and age. Your physician needs your help. Will you leave it all up to your physician? Or will you be a good partner, heeding the words of the poet Donne… And therefore never send to know For whom the bell tolls; It tolls for thee. *
In summary, patients and physicians should travel the pathway to partnership together. Patients can do their part by (1) preparing for the clinical visits, (2) understanding and adhering to their treatment agreements, and (3) educating themselves about risks, side-effects, and legal aspects of their care. It is a real challenge to treat chronic pain in this day and age. Your physician needs your help. Will you leave it all up to your physician? Or will you be a good partner, heeding the words of the poet Donne… And therefore never send to know For whom the bell tolls; It tolls for thee. *  James Patrick Murphy, MD, MMM is Chair of the Board of Governors -and Immediate Past President- of the Greater Louisville Medical Society, Medical Director of Murphy Pain Center, and an Assistant Clinical Professor at the University of Louisville School of Medicine. Dr. Murphy contributes to numerous publications, has presented before national and international audiences, and consults with a wide spectrum of agencies and individuals regarding pain, addiction, and the future of healthcare in our country. He is board-certified in Pain Medicine, Anesthesiology, and Addiction Medicine. * References and links pertaining to this article are provided in the comments. * This unofficial summary is my personal opinion. A full, official version of the final rule should be consulted for compliance purposes at: http://www.in.gov/legislative/iac/20141105-IR-844140289FRA.xml.html The Indian State Medical Association also has a summary available at: http://www.ismanet.org/pdf/legal/IndianaPainManagementPrescribingFinalRuleSummary.pdf
James Patrick Murphy, MD, MMM is Chair of the Board of Governors -and Immediate Past President- of the Greater Louisville Medical Society, Medical Director of Murphy Pain Center, and an Assistant Clinical Professor at the University of Louisville School of Medicine. Dr. Murphy contributes to numerous publications, has presented before national and international audiences, and consults with a wide spectrum of agencies and individuals regarding pain, addiction, and the future of healthcare in our country. He is board-certified in Pain Medicine, Anesthesiology, and Addiction Medicine. * References and links pertaining to this article are provided in the comments. * This unofficial summary is my personal opinion. A full, official version of the final rule should be consulted for compliance purposes at: http://www.in.gov/legislative/iac/20141105-IR-844140289FRA.xml.html The Indian State Medical Association also has a summary available at: http://www.ismanet.org/pdf/legal/IndianaPainManagementPrescribingFinalRuleSummary.pdf  And if you really want to explore the Indiana pain regulations in detail, there is no better source than the online guide: First Do No Harm, The Indiana Healthcare Providers Guide to the Safe, Effective Management of Chronic Non-Terminal Pain. http://www.in.gov/bitterpill/docs/First_Do_No_Harm_V_1_0.pdf * Hey Hoosier! Who’s your partner?
And if you really want to explore the Indiana pain regulations in detail, there is no better source than the online guide: First Do No Harm, The Indiana Healthcare Providers Guide to the Safe, Effective Management of Chronic Non-Terminal Pain. http://www.in.gov/bitterpill/docs/First_Do_No_Harm_V_1_0.pdf * Hey Hoosier! Who’s your partner?  * * *
* * *