3/15/2025 UPDATE – For the time being, the ALARM ACT initiative has been merged with HB 788, which was filed by Representative Kim Moser in the Kentucky General Assembly. For more information check out the KYSAM advocacy HB 788 website: https://www.kysam.org/news
Kentucky House Bill 788 supports increased access to buprenorphine by empowering Kentucky’s providers to treat patients with evidence-based care. Check out this 9 minute video of Dr. Murphy’s recent testimony in Kentucky’s capital city: https://www.youtube.com/watch?v=3lILI0x4TXo
The salient issues remain consistent with the ALARM ACT initiative, thus I’m keeping this post on the website to provide historical context supporting our efforts to save lives.

On average, overdose kills five Kentuckians every single day.
There is something simple you can do today to help.
A brief call to your legislators, asking them to support the ALARM Act, could help save thousands of lives.
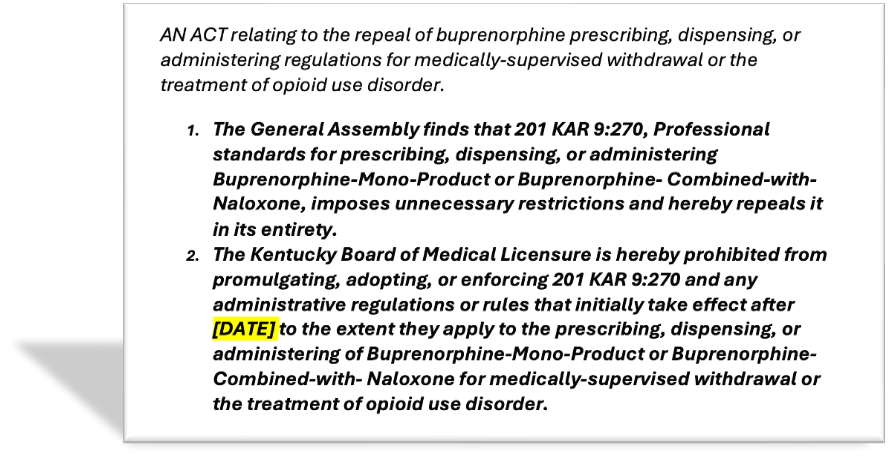
The ALARM Act is a legislative initiative aimed at improving access to buprenorphine – a lifesaving medication to treat opioid addiction – in fact, buprenorphine is our MOST EFFECTIVE measure to decrease overdoses and overdose deaths. The ALARM Act repeals regulation 201 KAR 9:270 – a decade-old KY law that severely hampers our doctors’ ability to prescribe buprenorphine.
Simply dial (800) 372-7181, and your message will be forwarded to your representatives.
You might say something to the effect of: Please help patients get the lifesaving medicine they need to treat addiction and prevent overdose deaths. Please support Dr. James Patrick Murphy and the Kentucky Society of Addiction Medicine by passing the ALARM Act, which repeal KY’s restrictive buprenorphine regulation 201 KAR 9:270.
Thanks! Now that you know my “ask,” please read on for the rest of the story…
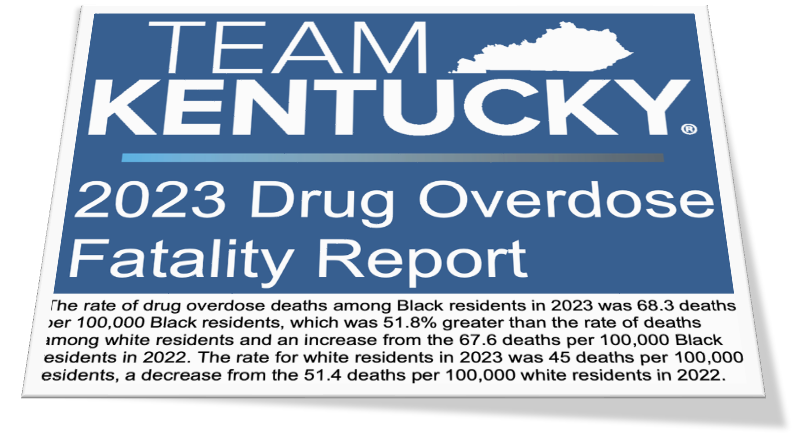
IN RECORD NUMBERS, KENTUCKIANS CONTINUE TO DIE FROM OPIOIDS.
Widespread availability of buprenorphine could decrease overdose deaths by 50% or more. Buprenorphine (sometimes know by the trade name Suboxone) is FDA-approved to treat damaged areas in the brain that cause opioid addiction and can prevent dangerous addictive behaviors that lead to overdose.
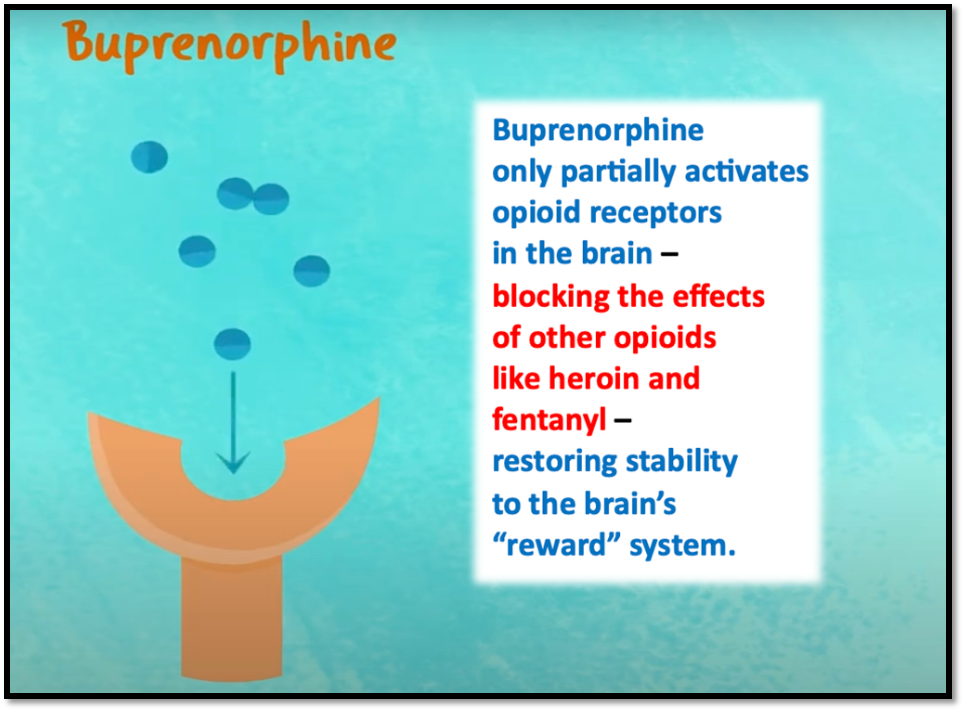
Distinct from NARCAN – which might reverse an overdose but does not treat the actual addiction –buprenorphine treats the root cause of the overdose. Buprenorphine promotes recovery, reduces crime, prevents overdoses, and saves lives.
Buprenorphine treatment is not simply trading one drug dependency for another. Quite the opposite, buprenorphine is a prescription medicine that treats the disease process, allowing patients to lead productive heathy lives – in much the same way that insulin allows people with diabetes to manage their disease and live well.
Tragically, barriers to accessing buprenorphine exist, such as regulatory burdens, costs, stigma, and unfounded fear of diversion. Thus, only one in five Kentuckians who need buprenorphine can get treatment.
In Kentucky, a major barrier to buprenorphine treatment is 201 KAR 9:270 – an obsolete law that is not aligned with current clinical evidence. This onerous regulation restricts effective dosing and forces doctors and patients to complete costly, unnecessary tasks and imposes unscientific mandates that contradict recommendations of the overwhelming majority of experts. This is beyond illogical – it’s dangerous and deprives suffering people of lifesaving medication.
Ask yourself, would anyone be OK with treating breast cancer this way? Of course not. So why is Kentucky so restrictive with treating ADDICTION ? – the #1 cause of death for adults under the age of forty.
Kentucky is a an outlier. Our federal government and most other states have already done away with antiquated regulations like 201 KAR 9:270, allowing buprenorphine to be regulated like any other DEA schedule 3 controlled substance – as it should be. But Kentucky, despite ranking among the absolute worst states in terms of overdose deaths, somehow is still hanging on to 201 KAR 9:270. This must change. The regulation must be repealed.
The ALARM Act is a vital grass roots legislative initiative, supported by the Kentucky Society of Addiction Medicine and many others, that will repeal 201 KAR 9:270 and allow all Kentucky doctors to confidently treat their patients with buprenorphine – the “gold standard” medication for treating opioid addiction.
Every overdose death is PREVENTABLE.
Sound the ALARM !
Contact Your Kentucky legislators and ask them to support the ALARM Act.
(800) 372-7181 Monday-Friday 7am to 6pm
or
(502) 564-8100 Monday-Friday 8am to 4:30pm,
And email addresses can be found on their individual bio pages:
Senators
Representatives
Ask them to help save lives by joining you in supporting the Kentucky ALARM Act.

James Patrick Murphy, MD, DFASAM
Email: doctormurphyglms@gmail.com