The premier offering of “Optimal Prescribing Is Our Inherent Duty” concluded on Sunday, February 9th. I plan on having more to say… soon.
For now, I thought it worthwhile to share the three emails I sent to our staff, participants, and faculty each evening.
It was a sincere privilege to serve with the OPIOID team.
FEBRUARY 7, 2014 – DAY ONE
Dear all OPIOID’ers,
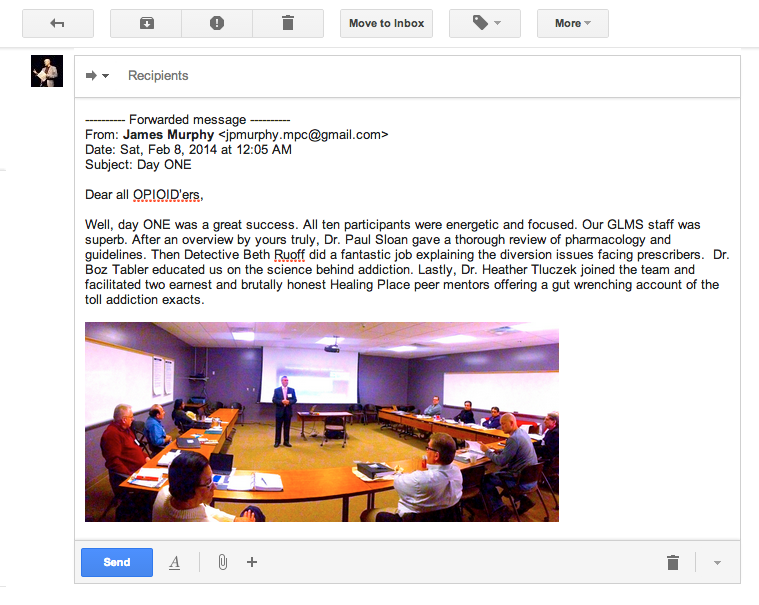
Well, day ONE was a great success. All ten participants were energetic and focused. Our GLMS staff was superb. After an overview by yours truly, Dr. Paul Sloan gave a thorough review of pharmacology and guidelines. Then Detective Beth Ruoff did a fantastic job explaining the diversion issues facing prescribers. Dr. Boz Tabler educated us on the science behind addiction. Lastly, Dr. Heather Tluczek joined the team and facilitated two earnest and brutally honest Healing Place peer mentors offering a gut wrenching account of the toll addiction exacts.

The staff of The Healing Place was great. The room was perfectly outfitted. And the food was delicious. And we ran on time all day! Thanks to Dr. Mary Helen Davis and Dr. Mark Boswell for stopping by for support… the day before they present.
Tomorrow (Saturday) we are at the Greater Louisville Medical Society headquarters for DAY TWO. More great lectures, discussions, and experiential learning! It’s happening! More later…
– Pat

FEBRUARY 8 – DAY TWO
Dear Friends of OPIOID,
Day TWO has come and gone… and what a day it was!

We convened bright and early at the Old Medical School Building (GLMS headquarters). After some camaraderie and a hot breakfast, Dr. Mary Helen Davis took us through the inner workings of KASPER, the governmental process involved in making policies, and finished with a discussion on physician motivation in the age of regulatory expansion.

We then had what, to the casual observer, must have looked like group therapy – led by Dr. Boswell Tabler. I believe this was another major breakthrough moment in the course, as the participants began to open up with personal accounts. At the end, all seemed to be fully motivated to make the changes necessary to be successful.

Then Dr. Ken Kirsh gave an extremely thorough review of the interface between pain and psychological issues. This was followed by Dr. Tabler’s interactive discussion on psychiatric treatment strategies.
After breaking for lunch, Dr. Mark Boswell had us enthralled by his categorical run down of the different types of challenging pain patients. He followed this with a lecture on how to screen for psychological pathology in our patient population.
Then it was on to “Pain Management Meets Speed Dating.” Dr. Heather Tluczek, along with Dr. Patrick Myers and seven other gifted actors posed as various types of challenging pain patient – allowing the course participants private one-on-one mock interviews. This was a fast-paced, exhausting, and enlightening experiential learning exercise. Everyone had a good time and learned something about themselves.
Tomorrow Dave Hopkins will get us up to speed on KASPER. Then I will be bringing it home with a thorough run down of Kentucky’s laws and regulations. We will conclude by getting familiar with some “tools” and memory aids in order to help the participants apply their new skills efficiently in their own practice setting.
This is going great! Our GLMS staff is fabulous. Our OPIOID faculty is superb. I almost don’t want it to end.
– Pat

FEBRUARY 9 – DAY THREE
Dear OPIOID friends,
In May of 2012, just after Kentucky passed House Bill One on the last day of a Special Legislative Session, the thought of having a comprehensive educational course for prescribers took root. Well, today that sapling idea bore fruit.
The inaugural OPIOID course concluded today around 1:00 pm. It was three days packed with lectures, group dynamic work, testimonials, didactics, theatre, poetry, and focused engaged effort by ten pioneering participants.

Today we had breakfast together then nourished our minds with 90 minutes of Dave Kasper, err, I mean Dave Hopkins – the KASPER director. He loaded our heads with vital information about our state’s electronic prescription monitoring program. I then led a discussion on drug screens and compliance monitoring. During our final two hours we poured over the Kentucky pain regulations in detail and learned strategies on how to incorporate the rules effectively into our daily practice routines.
What was most gratifying to me was seeing how our participants (now to be rightly known as our “partners”) remained focused and underwent a metamorphosis of sorts. But in reality, I don’t believe they were changed in any way by the course. Instead, I believe OPIOID may have rekindled a spark in each of them that was already there – only perhaps a bit beaten down by the regulatory grind. I know I was inspired by what happen over these past three days.
I am grateful to so many people and in the coming weeks I plan on communicating that message in other formats. For now, let me just say that everyone who participated – staff, volunteers, faculty, students, and even our impromptu professor GLMS security guard “Cory” felt something special had happened over the past three days.
…and something special has begun.
Yours in earnest gratitude,
– Pat

*still juggling…
patient
practice
community
*P.S. You had to be there.

James Patrick Murphy, MD, MMM is President of the Greater Louisville Medical Society.



 Phil and Pat, circa 1982
Phil and Pat, circa 1982