Success is counted sweetest by those who ne’er succeed.
~Emily Dickinson
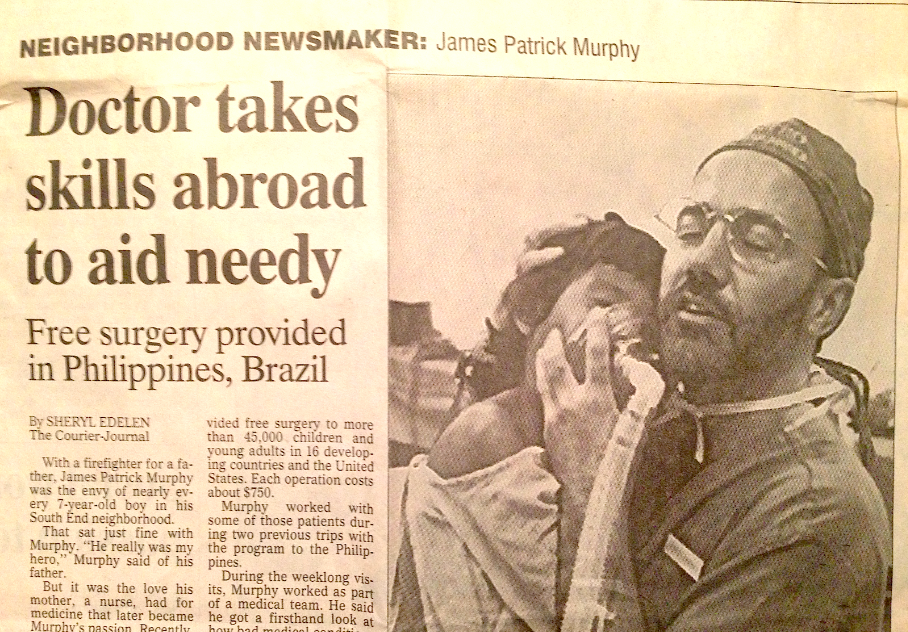
You treat chronic pain? Thank goodness someone does.
~My physician colleagues … on numerous occasions
I have treated chronic pain in a variety of practice settings, large and small, for almost thirty years. It has not always been easy. But I have found that success in this specialty is possible when the practice foundation consists of seven basic elements:
Cost-effective
Cooperation
Compliance
Consensus
Culture
Cause
Care
Chronic pain is not an exotic clinical niche. It is a chronic illness and should be approached step-wise as one would approach other chronic illnesses:
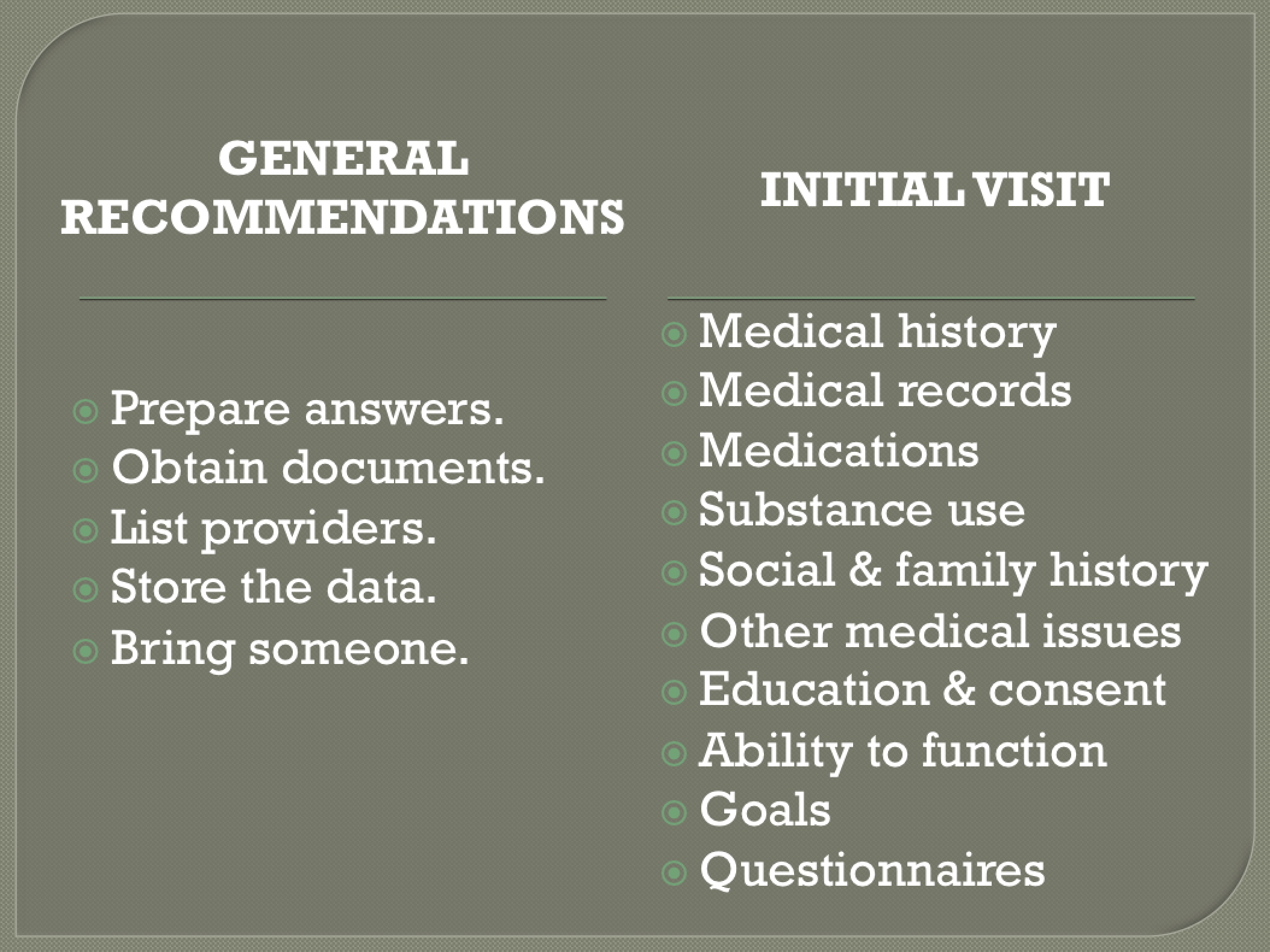
(1) Gather information;
(2) Make a diagnosis;
(3) Implement a plan of care;
(4) Assess the results; and
(5) Make adjustments.
A physician is generally comfortable with this paradigm when it applies to caring for an individual pain patient. However, regardless of one’s clinical confidence, when the practice’s primary mission is to treat chronic pain, overriding concerns about economic viability, community safety, and regulatory scrutiny become major stressors for a physician. More than just a paradigm is needed.
By embracing The Seven Essentials for Pain Practice Success a healthcare organization of any size or complexity can meet this need and provide quality pain care that is valued by the patient and professionally satisfying to the provider.
The Seven Essentials for Pain Practice Success
1. COST-EFFECTIVE
There’s no escaping the fact that healthcare costs are prodigious and resources are finite. Care providers may feel compelled to offer expensive treatments and order technologically advanced tests, regardless of the cost, out of a desire to provide the best care possible. But “best care” is not equivalent to “most-expensive care.” The success of any pain care practice is dependent upon use of resources – of the patient and the practice- in a manner that optimizes value.
2. COOPERATION
Do not tell patients what you will do to them. Instead, figure out how you can work with them. Providing care in a climate of draconian pain regulations, dogmatic practice guidelines, and dearth of evidence to support treatment options, is optimized by patient-practitioner partnerships. Success requires positive outcomes for the: (1) patient, (2) caregiver, and (3) community. If any of these three stakeholders have bad outcomes, failure is the sum total. With cooperation and teamwork, success is more likely achieved.
3. COMPLIANCE
Be a follower. In addition to an ever-increasing database of clinical guidelines, there are numerous regulations and statutes governing how healthcare providers may treat pain, particularly when treatment involves controlled substances. Some of the rules are federal statutes that apply universally. Other rules are only specific to individual states or communities. Rules governing pain care delivery may not necessarily reflect the best clinical practice, but are usually based upon sound principles. Search for the reason behind the rule. But if all else fails, go ahead and “teach to the test.” Compliance is mandatory. Even if you think “outside the box” do not act outside the box. Know the rules and follow the rules.
4. CONSENSUS
A successful pain practice must agree on how they will operate. Do some providers allow early refills, while others will not? Are some quick to discharge a patient who has an abnormal drug screen, while others give second chances? How often do we drug screen? Do we prescribe drugs on the first visit? Through honest communication the group must reach a consensus on “our way” of doing things.
5. CULTURE
Every organization has its own culture. A successful pain practice understands its culture, knows its weaknesses and knows its strengths. For example, if the group’s dominant culture is intuitive, then it needs safeguards (i.e. objective and detail-oriented policies and procedures) to focus on specifics. Success requires that individuals not only understand their roles, but also are willing to perform in a manner that supports the group’s dominant culture.
6. CAUSE
Successful pain practices know their cause, their mission, the reason the practice exists. Even the most mundane task can be passionately undertaken when team members understand how their actions contribute to the cause. In addition, successful practice managers make sure team members feel appreciated for their efforts.
7. CARE
Caring is the foundation for success. In all decisions, successful pain practices first ask: “Is it in the patient’s best interest?” Beyond that, every human encountered by the organization -patients, family members, hospital administrators, government regulators, insurance brokers, pharmaceutical representatives, colleagues, etc.- is worthy of dignity, respect, and care. The “golden rule” always comes before the rule of gold. Remember that no one cares how much you know until they know how much you care.
Each of the seven essentials for pain practice success is vital. Ignore one and the organization is on thin ice. Embrace them all and the practice, regardless of its size, can be on economical, clinical and ethical solid ground.
Then no one will have to “thank goodness” for what you do.
Instead, you can be thanked for the goodness that you do.
That is sweet success.
*

https://vimeo.com/channels/glms/68703810
James Patrick Murphy, MD, MMM is a Past President of the Greater Louisville Medical Society, Medical Director of Murphy Pain Center, and an Assistant Clinical Professor at the University of Louisville School of Medicine. He is board-certified in Pain Medicine, Anesthesiology, and Addiction Medicine and has a Master of Medical Management from the USC Marshall School of Business.
*Note: This article was originally titled: The Five Essentials for Pain Practice Success. “Cost-effectiveness” was added on July 30, 2015; “Cooperation” was added on September 30, 2015; each prompting a change in the title.
#
#
#






 https://jamespmurphymd.com/2014/03/18/is-there-method-to-this-march-madness
https://jamespmurphymd.com/2014/03/18/is-there-method-to-this-march-madness