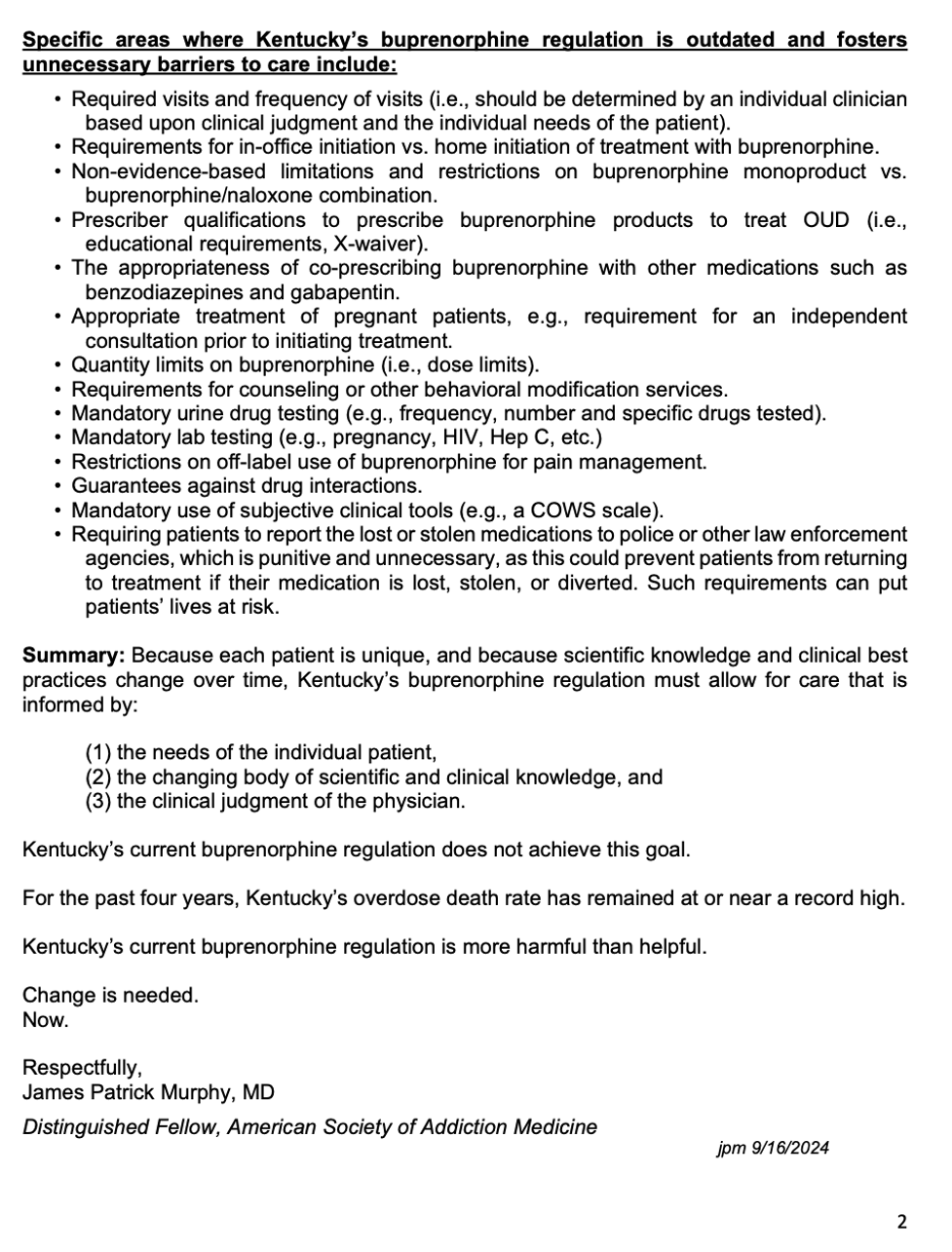
201 KAR 9:270 departs from acceptedstandards by imposing non-individualized requirements across multiple aspects of care, including
treatment initiation,
setting,
dosing,
formulation,
dispensing intervals,
co-prescribed medications,
drug and laboratory testing,
counseling and behavioral requirements,
consultations,
documentation, and
responses to perceived noncompliance.
These requirements delay, disrupt, or block care and impose disproportionate burdens on individuals with OUD, particularly those with transportation issues, housing instability, employment disruption, or childcare responsibilities.
disruption of care for patients with significant physical disabilities;
delays or denials for patients receiving other medically necessary medications;
delayed initiation or continuation due to mandatory specialist consultations;
avoidance of treatment due to perceived regulatory risk;
treatment interruption due to transportation, housing, or cost barriers; and
inability to initiate buprenorphine in emergency, acute care, or unhoused settings due to regulatory or institutional constraints.
The regulatory burden also deters physicians from providing addiction treatment in Kentucky and reduces clinician participation statewide.
The 2023 elimination of the federal X-waiver requirement under the Controlled Substances Act, together with the 2024 Federation of State Medical Boards’ statement affirming access to evidence-based treatment for opioid use disorder, further undermines the justification for the restrictive requirements imposed under 201 KAR 9:270, which are not aligned with prevailing national standards of care. These restrictions appear unnecessary to the safe regulation of buprenorphine given national standards supporting individualized clinical judgment in MOUD treatment.
During a recent state regulatory review, the American Medical Association, American Society of Addiction Medicine, Kentucky Society of Addiction Medicine, and American Psychiatric Association advised that failure to sufficiently amend 201 KAR 9:270 could undermine Kentucky’s response to the opioid crisis.
The Legal Action Center and Kentucky Equal Justice Center further stated the regulation may have a discriminatory effect on individuals with OUD by limiting access to evidence-based treatment based on stereotypes and assumptions rather than clinical justification, and may interfere with providers’ ability to deliver care consistent with ADA requirements.
A September 2022 Kentucky Opioid Response Effort (KORE) flier reported that buprenorphine reduces illicit opioid use and fatal overdose by over 50%. However, only approximately 20% of the estimated 150,000+ Kentuckians with OUD receive MOUD. Given this prevalence, 201 KAR 9:270 affects a substantial population that may be protected under the ADA. By conditioning access to buprenorphine on blanket regulatory requirements rather than individualized clinical judgment, the regulation creates statewide barriers to medically necessary care across settings and regions.
I respectfully request that the Department investigate 201 KAR 9:270 and consider enforcement action to remedy potential ADA violations. I will also submit supporting documentation by email.
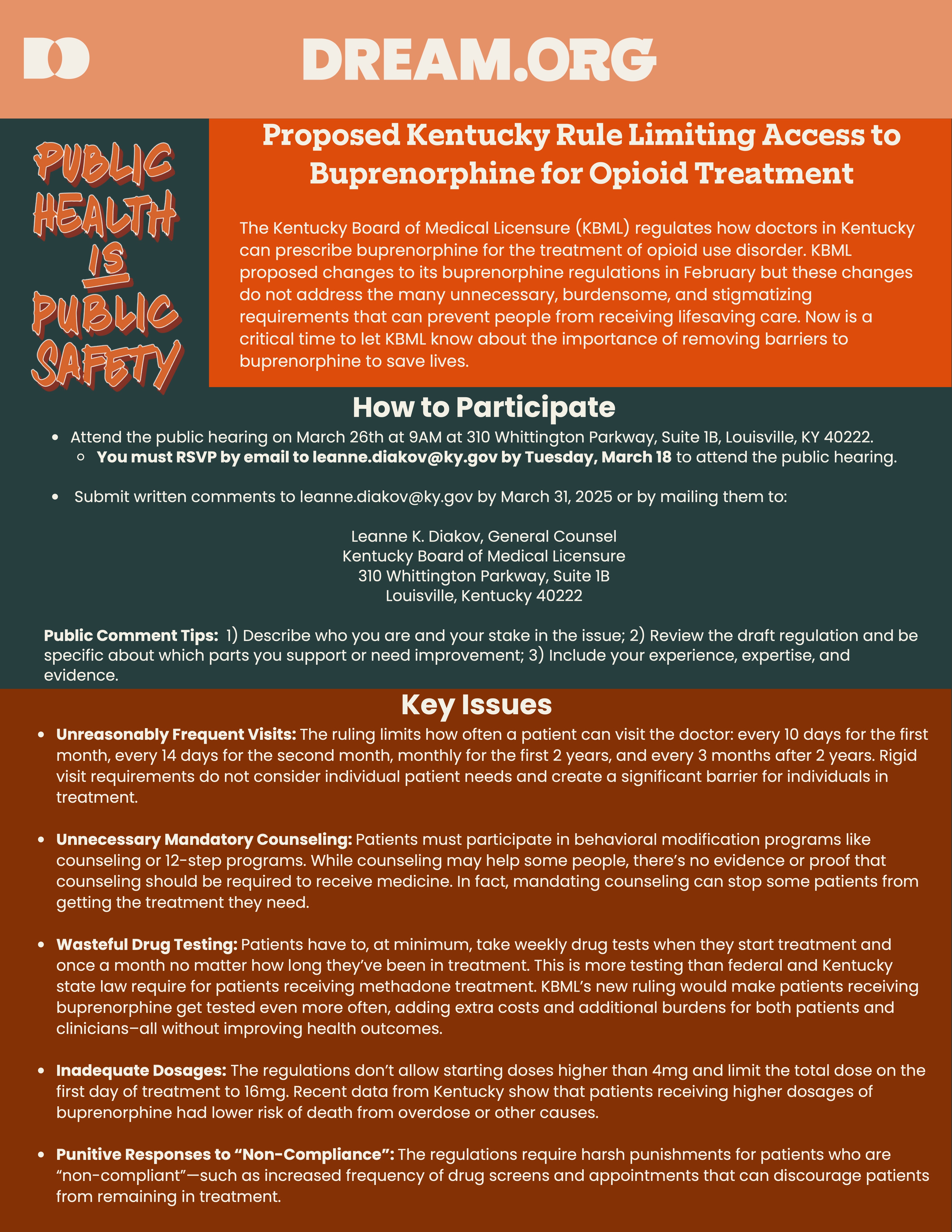
HERE’S THE LATEST: The Kentucky Board of Medical Licensure (KBML) filed their updated version of 201 KAR 9:270 (the buprenorphine regulation) and scheduled an in-person public hearing for March 26, 2025. However, KBML cancelled this hearing due to an overwhelming number of requests by speakers to be heard. KBML has now rescheduled the hearing for June 27, 2025, only this time it’s not in-person. It’s a Zoom meeting! They have not posted the link yet, so stay tuned and monitor the KBML website, link: https://kbml.ky.gov/Pages/index.aspx
Please mark your calendar for June 27th and spread the news. To review, below is a call to action from Dream.org sent prior to the cancelled March 26th hearing – NOW JUNE 27. The same issues are still at stake. Your voice is needed now more than ever! Even if you only Zoom in for thirty seconds. YOUR WRITTEN COMMENTS MATTER TOO! THANK YOU!
Dear Friends, Neighbors, and Colleagues,
Now is the time to take action! Your voice can make a difference in Kentucky. A simple email could help save lives. Here’s how: Send an email to the Kentucky Board of Medical Licensure (KBML) via
Leanne K. Diakov, KBML General Counsel at leanne.diakov@ky.gov
To make it easier, simply click on this LINK, where you’ll find a helpful brief to guide you in crafting and sending your email to leanne.diakov@ky.gov
NOTE: KBML HAS RESCHEDULED THE PUBLIC HEARING FOR JUNE 27, 2025, AND ARE ACCEPTING EMIALS AND WRITTEN COMMENTS THROUGH JUNE 27.
Tell KMBL that you do not support the proposed changes Kentucky’s buprenorphine regulation, and you believe Kentucky would be better served by eliminating the entire regulation known as 201 KAR 9:270.
The Kentucky Board of Medical Licensure (KBML) is nearing the final stages of updating the regulation 201 KAR 9:270, which governs the treatment of Opioid Use Disorder with buprenorphine in Kentucky. Even with the proposed changes, this regulation remains flawed and harmful, and KBML has yet to fully acknowledge the impact. You don’t have to take my word for it. Read it for yourself at https://apps.legislature.ky.gov/law/kar/titles/201/009/270/REG/
Unfortunately, KBML’s proposed amendments do not address the damaging, stigmatizing policies first introduced in 2015. But you still have time to help alter this course. Until JUNE 27, you can make your voice heard with an email to KBML.
Despite input from hundreds of specialists, caregivers, and concerned Kentuckians calling for significant revisions to this harmful regulation, KBML has moved forward with publishing insufficient amendments to their outdated regulations on buprenorphine prescribing. Sadly, these amendments do little to improve the situation and further create barriers for patients seeking this life-saving treatment.
Kentucky is out of sync with the rest of the country. While federal guidelines have simplified and streamlined buprenorphine prescribing in recent years, Kentucky remains one of the few states enforcing stricter, punitive measures. Kentucky’s buprenorphine regulation (and its proposed amendments) are not only unsupported by evidence but also contribute to an increase in overdose deaths by limiting access to care.
If 201 KAR 9:270 and its proposed amendments are allowed to proceed, Kentucky will miss the opportunity to align itself with thelatestscientificevidence, expertrecommendations, and current federal guidelines. Continuing with Kentucky’s flawed regulation will only result in more preventable overdose deaths in our state.
A ban on using buprenorphine-naloxone for chronic pain
It’s time to take action!
Now through JUNE 27, you have the opportunity to speak up on behalf of those struggling with opioid use disorder. Email your comments to:
Leanne K. Diakov, KBML General Counsel: leanne.diakov@ky.gov
At the end of this post, you’ll find a sample letter that you can modify to share your personal perspective, if you wish. Personalizing your message can make a big impact!
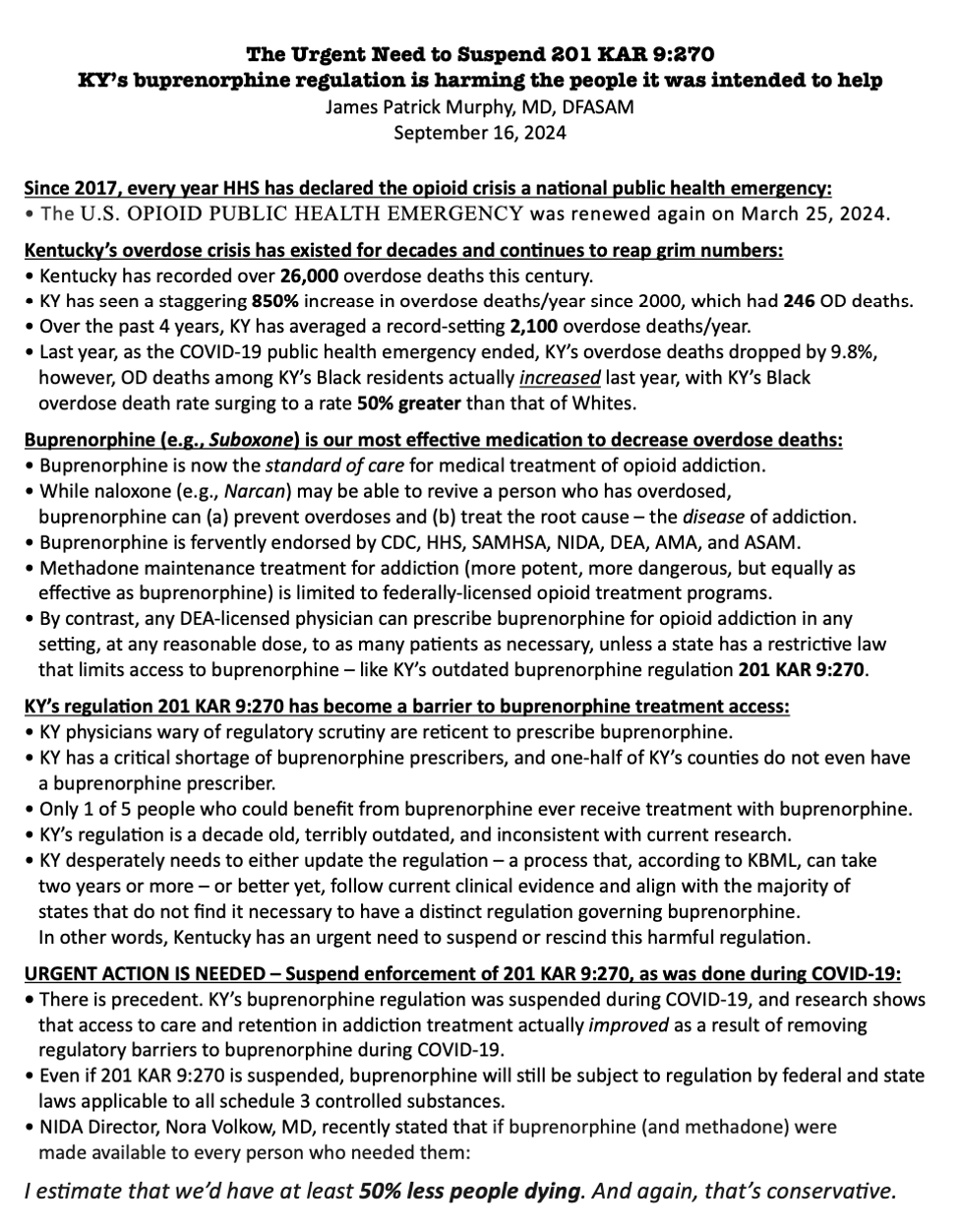
The Director of the National Institute on Drug Abuse stated that if everyone who needs buprenorphine could access it, overdose deaths could be reduced by half.
201 KAR 9:270 is a barrier preventing Kentuckians from accessing this life-saving medication.
And despite a tsunami of evidence proving the lifesaving effects of this medication, buprenorphine prescribing in Kentucky actually decreased last year! We must do better!
What more motivation do you need? Together, we can make a difference. Let your voice be heard!
Dr. Murphy is Kentucky’s Regional Director for the American Society of Addiction Medicine and is a founding member of the American Medical Association’s Substance Use and Pain Care Task Force. He serves as an Assistant Clinical Professor for the University of Louisville School of Medicine and is board-certified in Anesthesiology, Pain Management, and Addiction Medicine.
***SAMPLE TEXT***
To: Kentucky Board of Medical Licensure Attention: Leanne K. Diakov, General Counsel Email: leanne.diakov@ky.gov
RE: Public Comments on Proposed Amendments to 201 KAR 9:270
Dear Members of the Kentucky Board of Medical Licensure,
I am submitting my public comments on the proposed amendments to 201 KAR 9:270. Rather than addressing Kentucky’s overdose crisis, I am concerned that these proposed changes will only worsen the situation, creating additional barriers to care and limiting access to critical, lifesaving treatments. I respectfully urge the Board to prioritize evidence-based addiction treatment by rejecting these amendments and fully repealing this outdated and harmful regulation.
Expanding access to medications for opioid use disorder, such as buprenorphine, is crucial for reducing overdose deaths. Unfortunately, the proposed amendments directly contradict the guidance from several leading authorities, including the U.S. Department of Health and Human Services, the Drug Enforcement Administration, the Substance Abuse and Mental Health Services Administration, the National Institute on Drug Abuse, and the Federation of State Medical Boards, all of which support broader access to buprenorphine-based treatments. The restrictions outlined in 201 KAR 9:270 would be counterproductive and could exacerbate health disparities, especially within marginalized communities.
If these proposed amendments are enacted, 201 KAR 9:270 will continue to contribute to Kentucky’s tragically high overdose death rate. I fully support the concerns raised by the Kentucky Society of Addiction Medicine, which has reviewed the proposed changes and deemed them insufficient. In light of these concerns, I strongly advocate for the full repeal of 201 KAR 9:270.
Thank you for considering the potential impact of these amendments on the health and well-being of Kentuckians. I urge the Board to prioritize evidence-based addiction treatment by rejecting these amendments and fully repealing this outdated and harmful regulation.
Sincerely, [Your Name] [Your Credentials/Professional Title, if applicable]
Kentucky House Bill 788 (currently in committee) supports increased access to buprenorphine by empowering Kentucky’s providers to treat patients with evidence-based care. Check out this 9 minute video of Dr. Murphy’s recent testimony in Kentucky’s capital city: https://www.youtube.com/watch?v=3lILI0x4TXo
More and more people and organizations are joining this cause…
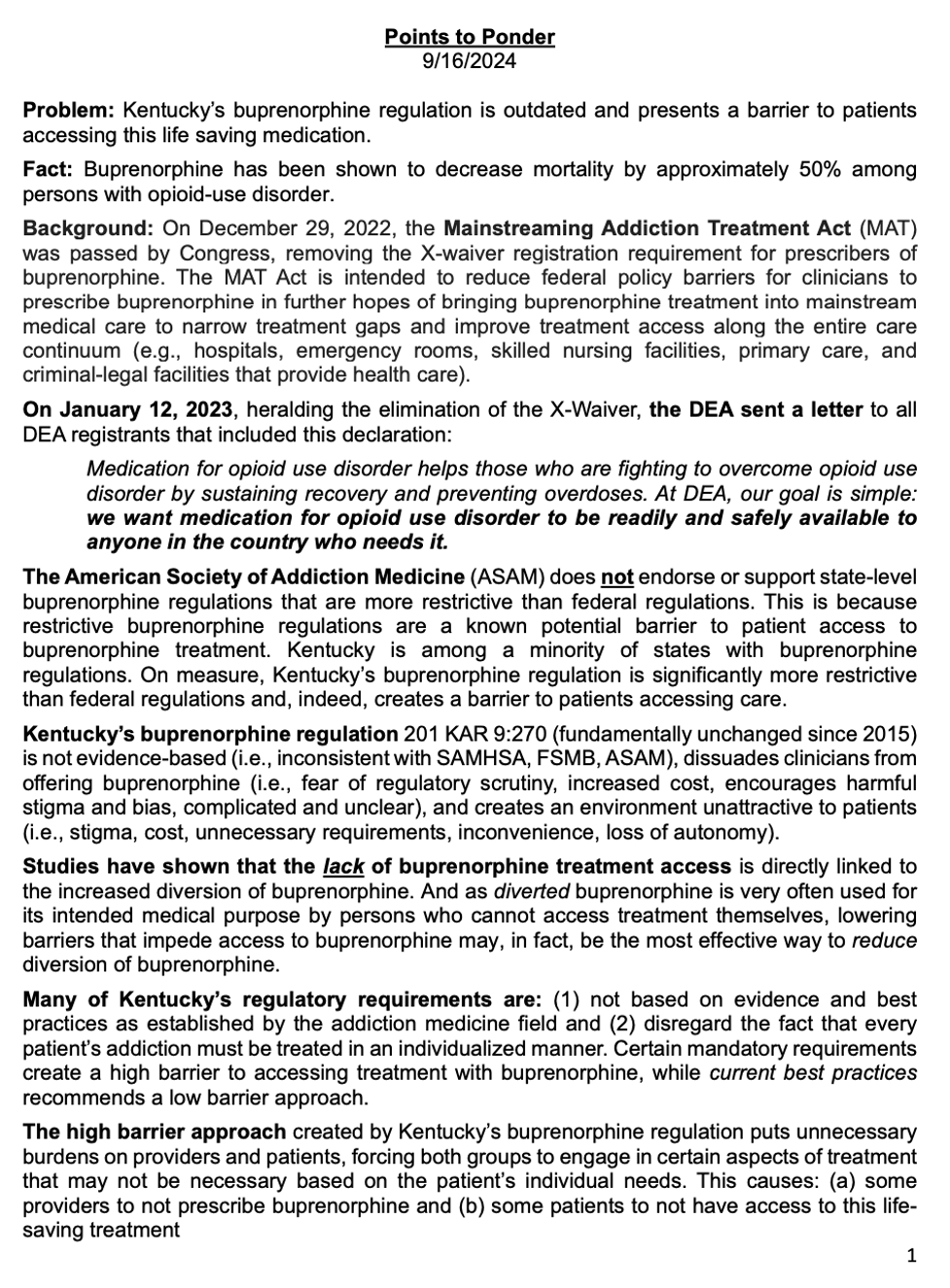
Buprenorphine is an FDA-approved medication for treating opioid use disorder, proven to be effective inpreventingoverdose deaths, reducing drug related crime, recidivism, and drug diversion, while saving valuable community resources.
However, Kentucky’s buprenorphine prescribing regulation 201 KAR 9:270 is outdated, unnecessary and harmful, because it creates barriers to accessing this lifesaving care.
Furthermore, despite all good intentions, this regulation paradoxically increases crime and diversion. Thus, for the safety of our communities, 201 KAR 9:270 must be repealed.
• Despite law enforcement, DEA, policy-makers, and medical experts universally calling for the removal of barriers to accessing buprenorphine, barriers continue to exist, e.g., stigma, costs, irrational fear of diversion, prescriber trepidation, and pharmacist and prescriber fear of regulatory scrutiny. 201 KAR 9:270 contributes to all of these barriers.
• 201 KAR 9:270 is a barrier to buprenorphine treatment, because it rigidly mandates actions that should be dependent on individual patient circumstances and prescriber clinical judgment; actions such as: frequent in-person evaluations, mandatory specialist consults, numerous urine drug tests, extensive labs, psychological counseling, outdated dosage limits, and irrational limits on medications for co-occurring conditions. Laws mandating such measures are not supported by scientific evidence, federal policies, or clinical practice guidelines from the American Society of Addiction Medicine.
• Frankly, Kentucky’s buprenorphine law 201 KAR 9:270 is years behind the times. To illustrate just how absurd it has become, consider that Kentucky requires a special DEA “X-Waiver” that doesn’t even exist anymore. On December 29, 2022, in an effort to increase access to buprenorphine, Congress eliminated all buprenorphine-specific federal regulations, e.g., the DEA “X-Waiver,” along with caps on the number of patients per prescriber, prescriber limits, mandated education. But 201 KAR 9:270 still requires prescribers to have the “X-Waiver.”
• In sum, Kentucky has perhaps the most outdated, draconian, and harmful buprenorphine regulation in our nation and is one of only 19 states that still have buprenorphine-specific regulations on their books. And sadly, prescriptions for buprenorphine in Kentucky have only decreased at a time when overdose rates are still at record levels. Repealing 201 KAR 9:270 is common sense.
Why is this so?
Because of rapidly evolving scientific and clinical knowledge, it’s impossible for policymakers to create regulations that strictly tell clinicians how to treat addiction with buprenorphine. Beyond that, Kentucky’s deliberate regulatory process is too slow and renders obsolete any attempt at reworking 201 KAR 9:270 even before the ink dries on the page.
Therefore, to save lives, reduce crime, and improve the health and well-being of our communities, please join the Kentucky Society of Addiction Medicine and support repeal of Kentucky’s buprenorphine regulation 201 KAR 9:270. This decade old law is outdated, unfixable, unnecessary, and harms the people it was intended to help. It mandates actions that are not supported by evidence, actions that inhibit access to treatment, actions that lead to increase drug related crime, and actions that promote fraud, waste, and abuse.
Rather than discourage drug diversion, 201 KAR 9:270 actually worsens drug related crime and diversion. And tragically, Kentuckians struggling with addiction are needlessly dying because of barriers to treatment caused by this law.
Repeal of 201 KAR 9:270 would allow buprenorphine to assume its rightful place in the category of DEA Schedule III medications with low risk, allowing clinicians to prescribe buprenorphine for its legitimate medical purpose in the usual course of sound professional practice. Make our communities safer and healthier. Repeal of 201 KAR 9:270 is critically necessary.
A summation of clinical, social, and scientific evidence, as well as expert opinion and federal policy focusing on DIVERSION, CRIME, and ACCESS:
Treatment with buprenorphine was associated with a REDUCTION IN ARRESTS, via Addiction Medicine, the official journal of ASAM. https://pubmed.ncbi.nlm.nih.gov/30916463/
Any steps taken to minimize buprenorphine DIVERSION and misuse must be careful not to undermine the positive patient and public health benefits gained from expanded treatment access, via University of Kentucky. https://pubmed.ncbi.nlm.nih.gov/25221984/
Barriers to treatment with buprenorphine include “Aggressive enforcement strategies by the DEA and several state attorneys general—including increases in raiding, auditing, and launching criminal investigations of waivered providers,” via National Academies of Science.https://nap.nationalacademies.org/read/25310/chapter/7#120
The Kentucky Medical Association (KMA), American Medical Association, and the American Society of Addiction Medicine (ASAM) support a bill (House Bill 121) that would remove insurance barriers to treatment with buprenorphine. The rationale supporting House Bill 121 (noted below) also supports the Kentucky Society of Addiction Medicine’s call for repeal of 201 KAR 9:270. For context, I encourage you to read the following “one-page” support document from the AMA:
For more information, please go to my blog CONFLUENTIAL TRUTH https://jamespmurphymd.com and start scrolling. Related stories begin with my post on June 28, 2024 about a petition to the Kentucky Board of Medical Licensure…
On Monday 9/16/2024, under a brilliant baking sun, from the south lawn of the state Capitol, Governor Andy Beshear proclaimed September to be Recovery Month in Kentucky. To his left and to his right sat about twelve sun-drenched dignitaries, most wearing business attire meant for air-conditioned offices. As I stood there in the front row, myself baking in the sun, I realized two things early on: (1) I had made the right decision to come, and (2) my game time decision to wear my UofL Med School polo shirt instead of a coat and tie was the right move (Can you find me in the pic below?).
Screenshot
I’d never heard Governor Beshear speak in person, and I found him to be as charming, personable, likable, and relatable as he always appears to be on TV. The governor said all the right things that needed to be said. He was inspirational as he recounted the work that had been done by Kentucky’s government over the past year battling the opioid crisis in our state. He touted KY’s 9.8% drop in overdose deaths from a year ago. He also said “There is a lot of work left to do.”
Eric Friedlander, Secretary of KY’s Cabinet for Health and Family Services also spoke and said he is thankful he is working for a Governor who “believes in science.”
And Lisa Lee, Commissioner for the Dept. for Medicaid, said that we’ve made progress, but she won’t be satisfied “until all barriers to treatment are gone.”
Others eloquently spoke, bills were ceremoniously signed, a few people with lived experience offered their compelling stories to the crowd, which dwindled a bit over time as onlookers gradually receded into the few shady spots farther away from the podium. All in all, the message was very positive. And as I stood in the front row to the right of the stage, facing Representative Kim Moser, the only other person besides me wearing red in Frankfort that day, I really wanted to believe the Governor when he said in closing, “I am convinced that we can defeat this epidemic.”
After the speeches, Representative Moser visited with me, offered me some of her views, gave me a little advice, and graciously invited me to come back to Frankfort in October to testify before her colleagues. She also introduced me to Secretary Friedlander, who I chatted with briefly. And before I left the podium area I got to speak with a true KY hero, Van Ingram, Executive Director for the Kentucky Office of Drug Control Policy.
These were all great connections to make. I had travelled to Frankfort thinking my main objective was to meet some of the people who I’ve been emailing regularly about the urgent need for a major overhaul of KY’s outdated and harmful regulation governing how physicians prescribe buprenorphine to treat addiction. I felt that my meet-and-greet mission had been accomplished. I could now report back to my organizations (i.e., KYSAM, ASAM, AMA, KYHRC) that our concerns about the buprenorphine regulation were probably a little closer to getting heard by the people who could bring about the needed change.
What happened next was unexpected.
I walked to the far end of the road between the Capitol and the Annex Building where dozens of addiction treatment, addiction recovery, and addiction support groups had set up tents, tables, and booths. I decided to visit every group represented there. I learned what they did, how they were funded, what role they played in the orchestra of helpers throughout our state. I met some amazing people, and I am definitely going to follow up with as many as I can. We truly have some fantastic advocates and caregivers in our state.
And maybe providence had a plan for me that day, because as I worked my way along that road from the far end to the beginning, near the humongous, beautiful, and famous floral clock on the Capitol grounds, the last group I visited was comprised of only two women. Out of respect for their privacy, I won’t go into specifics. But suffice it to say, these two amazing individuals were living fulfilling lives in recovery from opioid addiction, both were being treated with buprenorphine, and both told me that treatment with buprenorphine had literally saved each of their lives.
With this as my send off, I left the Capitol a little more sunburned but tremendously more inspired. It’s clear, there are a lot of wonderful people in our state doing fantastic things to help people with addiction make it to their promised land of recovery. And I’m more determined than ever to prove myself worthy of inclusion amongst the ranks of these dedicated and compassionate healers, by virtue of my doctoring, my advocacy, and my caring.
If you’ve read all the way down to this point in my article, then you are likely one of those wonderful people I mentioned in the paragraph above – because I know my writing is nowhere near as compelling as the cause. And you’re probably a person who wants to make a difference – maybe even save a life in the process. If so, then I have an ask of you…
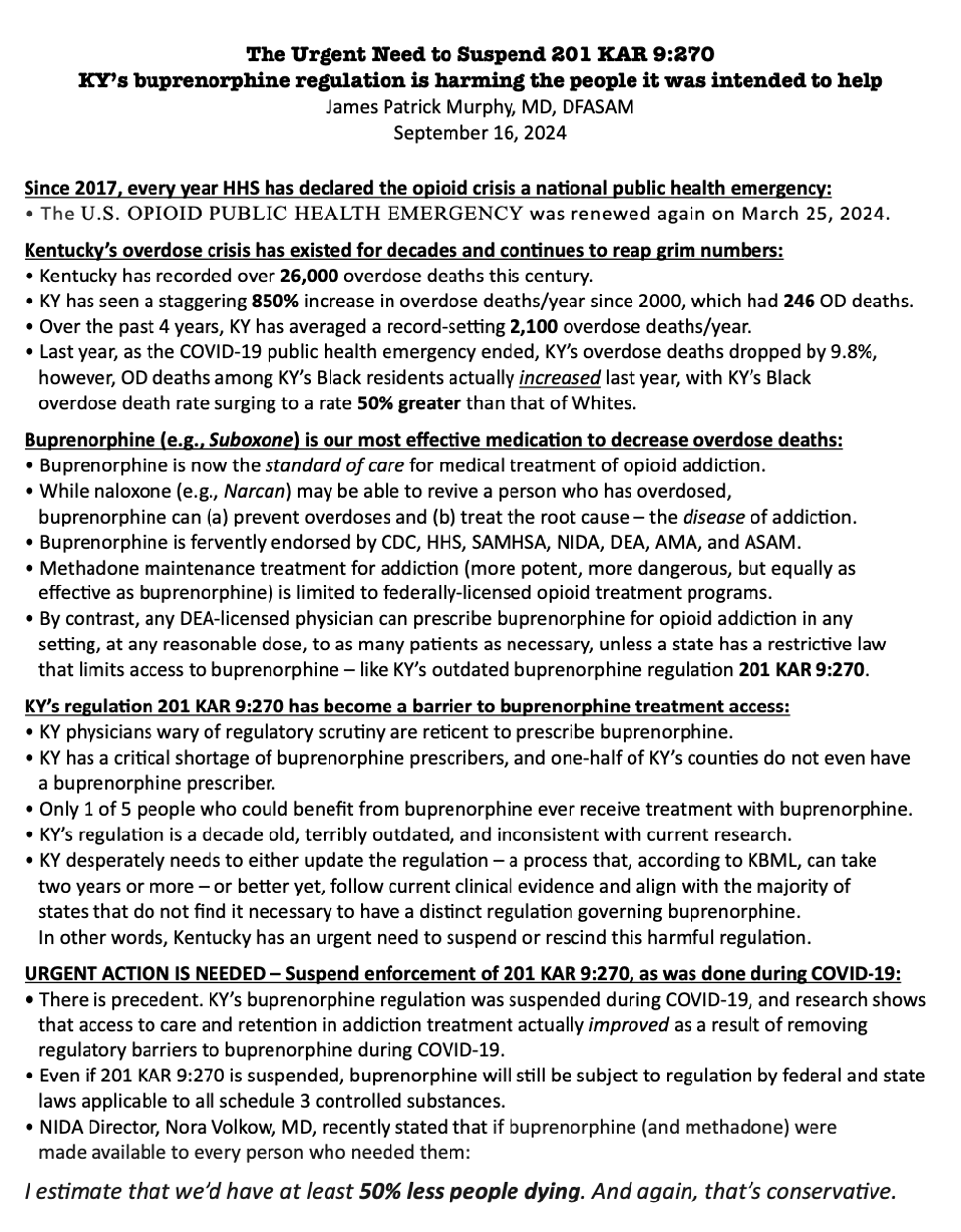
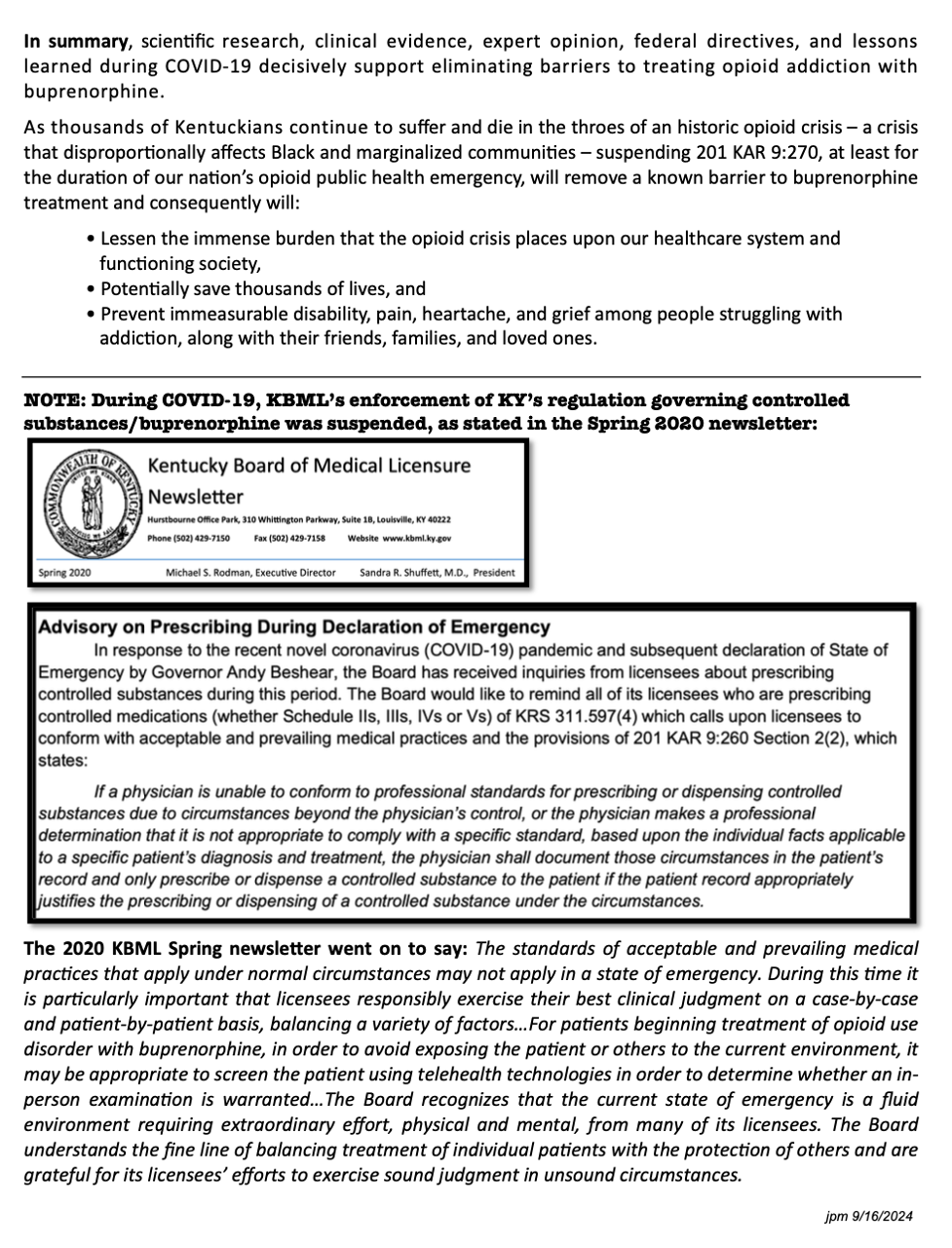
Please help me get the message to our Governor that Kentucky’s outdated buprenorphine regulation needs to be gone. The science, the data, and the lived experience of thousands in recovery confirm that buprenorphine treatment for opioid addiction promotes recovery, prevents overdoses, and saves lives. I made some handouts that I gave to people at the Recovery Month event on the Capitol lawn. Below you will find screen shots of the handouts.
As I said to one nice young lady, who politely told me that because she was employed by the state there was no way she could advocate for changing a state regulation, “That’s all right. I’m just asking that you read it.”
“Why?” she asked.
“Because, once you read it, you can’t un-read it.”
So, now I humbly ask you to please read the information below. And if you want to help remove a significant barrier to people with addiction receiving the most effective treatment we have to prevent overdoses and promote recovery, then stoke your creativity, ingenuity, determination, and problem-solving skills and help me find a way to get this information to Governor Beshear.
As Secretary Friedlander said, our Governor believes science.