Treating pain can be simple or complex.
The simple approach focuses on cause and effect.

Remove the cause of pain and the effect is…relief.
This often works when the cause is clear, i.e. acute pain. Just ask the lion with the thorn in his paw.
But chronic pain is often more complex.
Nature tries to smooth out rough spots; this is called “adaptation.” So when the brain is exposed to prolonged painful stimuli, or to foreign chemicals, such as opioid pain pills, the brain adapts.
Two examples of these neuroadaptations are:
(a) tolerance – the need for increasing doses to maintain the same effect; and
(b) physical dependence – the need to keep taking a drug to ward off withdrawal symptoms
The presence of drug tolerance and physical dependence does not mean the individual is addicted to the drug.
Addiction is a life-threatening disease of the brain’s reward circuitry, typified by a persistent destructive preoccupation with satisfying an unhealthy craving for a substance or behavior.

Addicts will often develop tolerance to drugs of abuse and develop physical dependence. And they experience withdrawal symptoms when these drugs are leaving their bodies. But tolerance and physical dependence (and withdrawal symptoms) are normal expected physiologic adaptations that can also occur in non-addicted people who take their medications as prescribed.
Furthermore, in the American Psychiatric Association’s authoritative Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, tolerance and withdrawal symptoms are no longer counted as criteria for diagnosis of substance use disorders when occurring in the context of appropriate medical treatment with prescribed medications.
In pain sufferers exposed to opioids for an extended period of time, drug tolerance and physical dependence can extend to brain structures that control stress, anxiety, pain, memory, emotions, judgment, critical thinking, and even the ability to experience joy. These patients may not be addicts, but if and when they are in withdrawal they sure feel like addicts. They may need the opioid for more than just pain relief; they may need the opioid just to feel “normal.”

If not addiction, then what is this complex neuroadaptation to long-term exposure to opioids? In a 2012 commentary article from JAMA Internal Medicine, Doctors Ballantyne, Sullivan, and Kolodny referred to it as “complex persistent opioid dependence” (JAMA Internal Medicine September 24, 2012, Vol 172, No. 17):
Dependence on opioid pain treatment is not, as we once believed, easily reversible; it is a complex physical and psychological state that may require therapy similar to addiction treatment, consisting of structure, monitoring, and counseling, and possibly continued prescription of opioid agonists.
I concur.

For years in my practice, my colleagues and I have treated chronic pain patients, many of whom are stable and functioning well on opioids. Interestingly, many will describe their pain as severe (i.e. “ten out of ten”) but in the same breath say they are doing “OK.” We have had a measure of success at tapering some patients to lower opioid doses, but a significant number simply will not function well at lower doses.
How can this be?
I believe the answer is in their neuroadaptation. To my understanding, long-term pain coupled with long-term opioid use appears to alter the way one’s brain experiences pain. It is almost as if the pain level is “locked in” and will not fluctuate significantly regardless of interventions (e.g. physical therapy, biofeedback, injections, adjunctive medications, or even more opioids). In this sense it is similar to how a patient with phantom limb pain can have real pain where the limb once was. In both situations the pain experience is determined by complex interactions between multiple nerve pathways – far from simple cause and effect.
Therefore, when treating complex persistent opioid dependent patients (“CPOD”) the most beneficial course might be to shift focus from the conventional drumbeats of: (a) trying a steady progression of new treatments; and/or (b) tapering off the opioids “at all costs.”
I would never suggest these pain patients abandon efforts to achieve more relief and improved function. But I am suggesting, as do Doctors Ballantyne, Sullivan, and Kolodny, that the better therapeutic approach may be to view their care through the lens of Addiction Medicine in addition to that of Pain Medicine.
CPOD patients might be well served by care plans influenced by principles outlined in The ASAM Criteria from the American Society of Addiction Medicine.
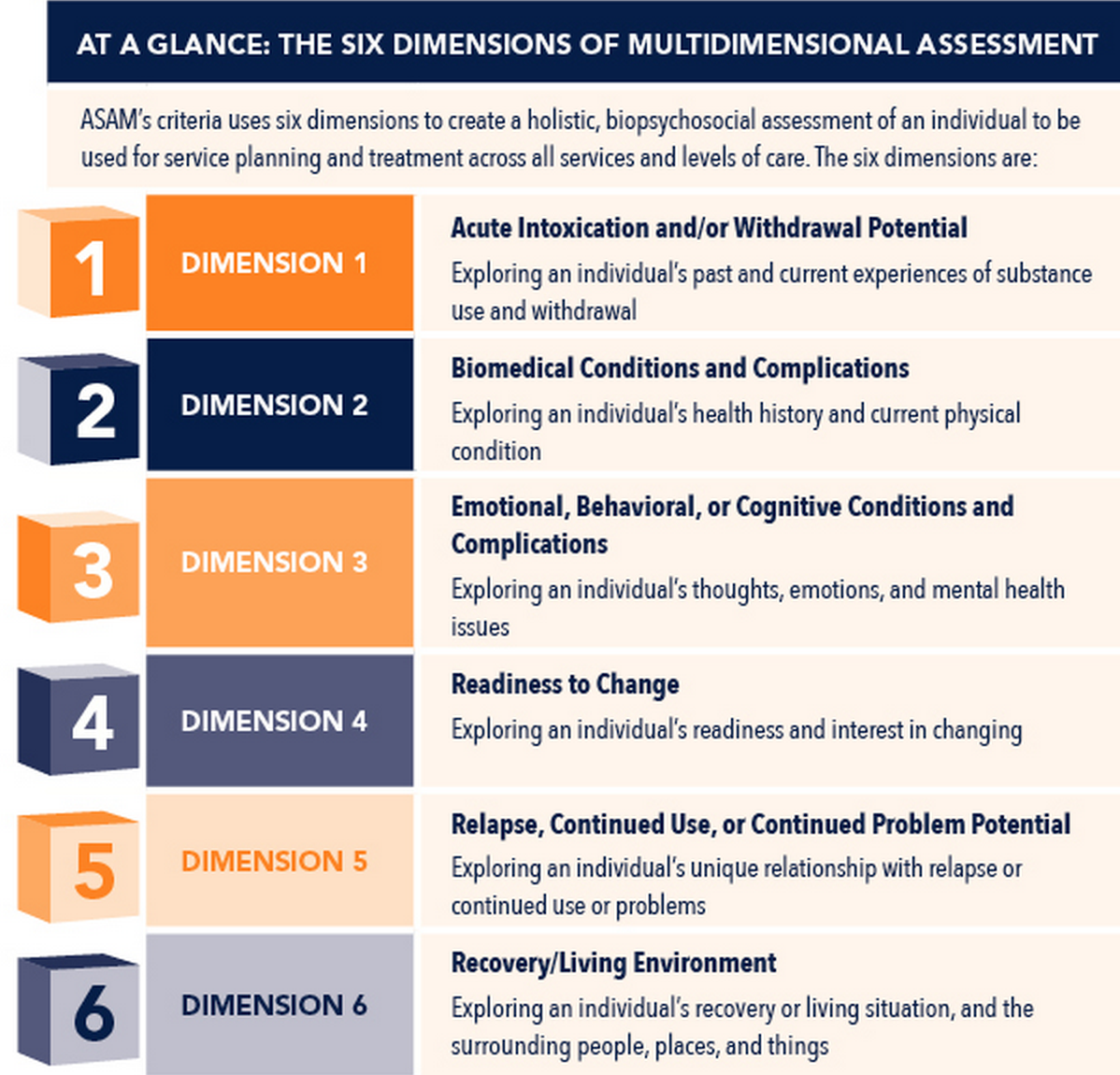
In this paradigm a patient is assessed in six categories or “domains.” Care plans are determined by severity in each domain. With CPOD patients the six domains would look like this (i.e.,“ABC & RRR”):
- Acute issues
- Biomedical issues
- Cognitive and behavioral issues
- Readiness to comply with the program
- Relapse potential to aberrant behaviors
- Recovery environment for ongoing safe use of opioids
Consideration of these six domains assists the clinician in formulating a treatment plan with the most appropriate structure, monitoring, counseling, and use of opioid medications.
For example, imagine a patient with chronic pain who presents for continued use of opioids and is assessed to be stable in five domains but has not adequately addressed his or her diabetes. The diabetes is a biomedical issue that left untreated could jeopardize safe use of opioids. In order to move forward with the plan of care, optimizing this “biomedical” domain becomes a priority.
Treating pain can be simple or complex. When the cause of pain is known and removing the cause is expected to result in pain relief, the decision whether or not to include opioids in the plan of care is straightforward. However, when long-term suffering and opioid use lead to significant neuroadaptations and the development of complex persistent opioid dependency, the best course of action may be to offer these non-addicted pain patients a plan of care modeled after that which has been shown to be effective in treating addiction.
Those afflicted with the disease of addiction suffer biological, psychological, and social harm. Respect, dignity, and science are the pillars of treatment. Success requires ongoing partnership between the patient, caregiver, and support group.
This plan of care can also work well for complex persistent opioid dependent pain patients. They may not be addicts…But you can treat them that way.
Simple.

*
*
*

Nice work Dr. Murphy. Clearly as you point out, it takes a while neighborhood to treat persistent complex pain, and the patient themselves are front and center!
Here is the text of one of the first articles I ever wrote concerning ways physicians can prevent prescription drug abuse. It was published in “Louisville Medicine” (March 2004) – the official journal of The Greater Louisville Medical Society. Most of this still applies today…
*
*
*
March 20, 2004 Article: Controlled Substances Task Force
James Patrick Murphy, M.D., Chair, Controlled Substances Task Force
“This is may be the most unusual place you have ever telephoned,” I said, responding to a call last October by Dr. Gordon Tobin, Jefferson County Medical Society (JCMS) President. At the time he contacted me, I happened to be standing atop the Washington Monument, looking directly at the Justice Department Building (the “D.E.A.”). What had prompted Dr. Tobin’s call was the news that yet another JCMS physician had had his license suspended by emergency order of the Kentucky Board of Medical Licensure due to issues directly related to the prescription of controlled substances. Now the occasional license revocation here or there does not seem to make much of a news splash, but this was the second JCMS physician in two weeks to have his or her name plastered across the evening news due to alleged controlled substance indiscretions.
Enough.
We have unfortunately grown accustomed to reading articles about shady narcotic prescription-writing practices in rural areas of Kentucky. But it seems the authorities are now turning their attentions toward physicians in the “16th largest city in America.” Sergeant Bill Stivers head of the Louisville Metro Police Prescription Drug Squad has indicated to me that the best motivation for people making correct decisions is to hold them accountable for their actions. He feels that the problem of prescription drug abuse is “neither new nor phenomenal” and that addressing the problem at its source (i.e., physicians) is critical. Sgt. Stivers recently wrote to me: “Prescription drug fraud/abuse has been a major element of the narcotic problem for years in the United States. The only ‘new’ issue is the attention that the problem is now receiving. The attention may be highlighted by the newer more technologically advanced (potent) medications and the larger number of controlled substances now available. The problem has been with us for many years. The fact that more people are now dying due to prescription drug fraud/abuse is the only ‘new,’ albeit unfortunate, result.”
Enough.
Prescription drug abuse is a problem of epidemic proportions in Kentucky as well as in the rest of the country. According to the American Pain Foundation, up to 75 million Americans are afflicted with pain (1). Abuse and dependency in chronic pain patients has been shown to range from 3.2% to 45% (2,3). The 2000 National Household Survey on Drug Abuse recorded that in 1999 an estimated 9 million people aged 12 and over used prescription drugs non-medically. Nearly 3% of all Kentuckians surveyed that year admitted to illicit drug use other than marijuana (4). Also, the number of Americans who for the first time used pain relievers non-medically was three times the number of people who did so in the mid-80’s. Emergency room visits resulting from narcotic pain relievers abuse have increased 163% since 1995.
Unlike most drugs, controlled substances are not “owned” by clinicians. The utilization of antihypertensives, birth control pills, insulin, and other “non-scheduled” drugs is generally confined within the sanctity of the doctor – patient relationship. However physicians share their dominion over controlled substances with regulatory agencies (i.e.: DEA, police, medical boards). These drugs have uses that are decidedly non-medical and decidedly illegal. These “other uses” are a big business for illicit dealers and a big problem for society. Police are being shot, young people are dying at parties, relationships and lives are being ravaged in a parallel universe with cancer and chronic pain patients who need these medications to “salvage” their lives.
Enough.
More and more politicians and public officials seem to be staking their reputations on addressing drug abuse in Kentucky. According to stories from the media, both Lt. Governor Steve Pence and Attorney General Greg Stumbo have made curbing drug abuse the number one priority of their new administrations. There seems to be a new agency or bureau formed each month whose aim is to address this issue. The Kentucky Board of Medical Licensure has asked for even greater authority to extend use of the KASPER (Kentucky All Scheduled Prescription Electronic Reporting) system, now primarily utilized to investigate patients, to the investigation of doctors as well as their associates, partners, and even their peers residing in the same locale ( Kentucky SB-14). This year the federal government has added “over prescribing of Oxycontin” to the short list of occurrences that can trigger an audit for fraud and abuse.
The practice of medicine is constantly evolving, and so are the laws that govern the manner in which physicians are allowed to practice. Regulatory agencies are partners with physicians, while at the same time are “consumer advocates” charged with protecting the public from transgressors of the law. The regulatory agencies’ role sometimes places them at odds with physicians. There certainly are some physicians who run prescription “mills” for huge profits with little clinical justification for their actions, and they should be investigated and penalized. As for the disreputable physician who knowingly engages in criminal activity, he or she should obviously be prosecuted. But what about the honest physician who is simply applying clinical knowledge learned in medical school and is not fully aware of the evolving non-clinical responsibilities? This physician may get “caught” prescribing controlled substances without adequate documentation and outside the bounds of “acceptable medical practice.” With KASPER and the DEA computer systems, physicians can be monitored and “trended” and as a result investigated. Whether we like it or not, we are being watched.
Pain is the most common reason people seek the advice of a physician. Treating pain is the most basic task physicians perform. Morphine has been in use for about 3500 years and is still the most commonly prescribed pain medication. Unfortunately many physicians choose to avoid using opioids out of fear of falling under the veil of an investigation.
Coach Rick Pitino of the University of Louisville Cardinals has talked about his players being intelligent but having varying degrees of “basketball IQ”. Likewise, physicians need to have “controlled substance IQ” above and beyond clinical knowledge in order to win against those who would try to abuse and divert the medications, in order to withstand the scrutiny of regulatory agencies, and in order to adequately treat pain.
It used to be “document, document, document,” were the buzz words. Clear documentation remains necessary, but our actions must speak at least as loud as our words. “Do” is the first part of documentation. The following are the Top Ten Actions a physician can do in order to elevate controlled substance IQ.
1. Download the Kentucky Board of Medical Licensure guidelines for prescribing opioids. Follow them. Post them in your office. Be able to quote them. We are fortunate that our board’s guidelines are comprehensive, up to date, and nationally recognized as such. The website is: http://www.state.ky.us/agencies/kbml . The U.S. Federation of State Medical Boards (www.fsmb.org ) contains the basic guidelines that most states (including KY) have adopted. The Maryland Board of Physicians has a very good videotape presentation regarding the lawful prescription of controlled substances which can be obtained by calling 800-492-6836. Any “ consumer” can trigger an investigation by the Board. The law dictates that all controlled substance related complaints must be investigated. If you are fearful of an investigation, you probably should not be prescribing opioids.
2. Get to know the police in your jurisdiction on a first name basis. Do not bully them or treat them with “I know what is best” arrogance. Invite them to give a seminar to your staff. When they offer suggestions, use them. Our Police Department’s “Awareness Through Education” program is aimed at building bridges of understanding and opening crucial lines of communication between police and medical professionals. It is an outstanding program. Contact Sgt. Bill Stivers at (502) 574-8617 to arrange a seminar. For additional helpful advice, visit the DEA website at http://www.deadiversion.usdoj.gov/pubs/brochures/drugabuser.htm .
Know the law (5). The laws have been changing rapidly over the last 5 years. Do not pre-sign blank prescriptions. It is not just a bad idea, it is illegal (felony). Do not write prescriptions for controlled substances for yourself, your family, or your staff. Get the KMA Legal Handbook for Kentucky Physicians 2004 by calling (502) 426-6200 or by logging on to their website: http://www.kma.org . As a physician you can also join the National Association of Drug Diversion Investigators (www.naddi.org) .
3. Employ measures to document patient compliance. Obtain prescription utilization reports (KASPER). KASPER requests are available by calling (502) 564-7985. Order or perform urine drug tests. Understand drug testing and its limitations. (6). A free CME program regarding drug testing is available by calling Purdue Pharma (203-588-4479). Perform random pill counts. Try to make these measures seem supportive rather than punitive. Promote an upbeat “culture of compliance” in your office as opposed to a suspicious and punitive environment.
4. Proper patient selection is crucial. Screen patients and choose wisely which ones can safely be given opioids. No single test exists that is sensitive enough to detect everyone who might abuse opioids. Patients may be less than truthful in answering questions. Testing can, however, open the door to meaningful dialogue. Use standard and accepted assessment tools. Examples for substance abuse issues are: CAGE Questionnaire (7) (www.palliative.org/pc/clinicalInfo/AssessmentTools/Cage.pdf) and DAST – 10 (www.nova.edu/~gsc/online2/DAST10.doc) . SASSI drug and alcohol abuse screen, BECK Depression Scale, and the Personality Assessment Screener (PAS) are each easy to use, meaningful, inexpensive and can be obtained from Psycorp (800) 872-1726. When in doubt, send the patient for a formal psychological evaluation and / or addiction screen. The local police will do background checks for a small fee (502-574-2050) or for a more thorough check statewide call (800-928-6381). You literally cannot know too much about your patient. Accept the fact that some patients simply should not receive opioids.
5. Do a thorough history and physical examination that documents the reasons the pain exists, not just that the pain exists. “Build a case” for your patient’s needing opioids. Obtain old records. Talk to the patient’s previous physicians. Imagine that every patient is an undercover DEA agent (he might be), and document your rationale for your decision to use opioids. Follow up frequently and address the “4 A’s” in you notes: Analgesia level, Activity level (function), Adverse side effects, and Aberrant behavior. (8). Keep legible and complete records.
6. Do not go it alone. Get a second opinion. As with any complicated disease process, if it is not covered in your specialty, ask for a consult. Find someone who you trust who either agrees with your management or whose advice alters your course of treatment for the better.
7. Use narcotic agreements and obtain informed consent. Follow up on “breaches” of the agreements. An example of such an agreement can be found at http://www.osbn.state.or.us/pdfs/pain.pdf .
8. Prescribe in a logical manner (9). Document reasons for each change. Start low and go slow with dosing. Do not escalate dosage once the patient is stable. Limit “breakthrough” dosing. Use timed-release opioid preparations when appropriate (10). Use the least amount of medication possible. Establish realistic expectations and goals. Document function and progress toward goals periodically (11). Write for limited quantities. When in doubt the first actionto consider is to give out less medication. Avoid phoning in prescriptions of schedule III and IV opioids. Write the amount prescribed in long hand, not just numerals. Include the patient’s address on each prescription. Create a “hard copy” of prescriptions and keep a copy for your records.
9. Communicate with the rest of the health care team and your patient’s support group. Get everyone on the same page regarding goals and treatment plans. Get to know the pharmacists. Have your patients use only one pharmacy for their opioids (KBML)
10. Document that you have had CME regarding the prescription of controlled substances. Attend meetings. Learn from your pharmaceutical reps what resources are available. CME is available free of charge from many organizations such as the National Pain Education Council ( http://www.npecweb.org ). Join an organization such as: the American Academy of Pain Medicine, American Academy of Pain Management, and the American Pain Society. Participate in our JCMS task force.
There certainly are many other suggestions which can be helpful. However, if you put into practice the basics from the above list you will be doing your part as a responsible member of the coalition battling prescription drug abuse.
Regulatory agencies, police departments, and health care providers share the same goal — keeping medications in the hands of the patients who need them and keeping them out of the hands of the people who abuse them. In an effort to be proactive the Jefferson County Medical Society has formed a Controlled Substances Taskforce.
Our JCMS task force does not intend dictate how anyone must practice medicine. The purpose of our task force is ultimately to improve health care for our patients and to support our physicians’ efforts to achieve that end. Our major emphasis is on education for physicians, patients, and the public at large. Our task force is working with the board of licensure, police agencies, government agencies, pharmaceutical companies, the media, as well as the traditional “health care team” of doctors, nurses, and pharmacists. Our task force will make every effort to inform our physicians about regulatory agencies’ expectations in the event of an investigation, thus alleviating anxiety accompanying such scrutiny. There will be public forums, printed materials, videotapes, and continuing medical education credits offered. Our member physicians will have the opportunity to display, for deserving patients, would-be drug abusers, and regulatory agencies, tangible documentation of his or her commitment to attacking the drug problem.
In the coming months our task force will continue to take shape. We welcome anyone and everyone’s input. If you are interested in helping in any capacity or just want to render an opinion or concern, please contact the JCMS at ______ or email _________ .
Enough is enough. Now is the time for action. Stay tuned.
References:
1.American Academy of Pain Medicine, A Brief Guide to Pain Medicine, 1996.
2. Dunbar, SA and Katz, NP. J Pain Symptom Management. 1996;11(3): 163-171.
3. Manchikanti L, et. al. “Prevalence of Prescription Drug Abuse and Dependency in Patients with Chronic Pan in Western Kentucky.” J Ky Med Assoc. 2003 Nov; 101, pp. 511-7.
4. Blondell, Richard D., et al. “Is The Kentucky Prescription Reporting System Useful in the Care of Hospitalized Patients?” J Ky Med Assoc. 2004 Jan (102).
5. Cole, B. Elliot. “Prescribing Opioids, Relieving Patient Suffering and Staying Out of Personal Trouble with Regulators.” The Pain Practitioner, Vol. 12, No. 3
6. Fishman, SM et al. “Adherence Monitoring and Drug Surveillance in Chronic Opioid Therapy.” J Pain and Symptom Management Vol. 20, No. 4 October 2000.
7. Buchsbaum, D.G., “Screening for Alcohol Abuse Using CAGE Scores and Likelihood Ratios.” Ann Internal Med 115(10), 774-7 (1991).
8. Passik, SD, and Herman Weinreb. “Managing Chronic Nonmalignant Pain: Overcoming Obstacles to the Use of Opioids.” Advances in Therapy, Vol 17, No.2, March/April 2000.
9. “Management of Cancer Pain, Clinical Practice Guideline, Number 9.” U.S. Dept. of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research: March 1994:12, 49-137. AHCPR publication no. 94-0592.
10. Arnoff GM: “Evaluation and Treatment of Chronic Pain, edn 3. Edited by Aronoff, GM. Baltimore: Williams & Wilkins; 1999: 433-453.
11. Ballantyne, Jane C., and Jianren Mao. “Opioid Therapy for Chronic Pain” NEJM 349;20, November 13, 2003.
*
Note: My posting of this comment was prompted by a blog article authored by Dr. Jeffrey Fudin: http://paindr.com/physicians-dread-it-pharmacists-dream-of-it-tackling-the-opioid-epidemic-analgesic-toxicity-by-collaborating
Tonight I added a “?” to the title of this blog post.
I have been reading comments, and it seems some people have focused on a negative connotation, misinterpreting the point I was hoping to make.
Addiction and chronic pain are both disease states. For that matter, so are diabetes, hypertension, HIV, and a host of other conditions. And everyone who battles chronic illness should be treated with dignity, respect, compassion, and with scientifically sound modalities. Thus addicts should be treated like pain patients and vice versa.
More specifically, since there is considerable overlap in some symptoms and ramifications associated with addiction and chronic pain, I have found the paradigm devised by the American Society of Addiction Medicine (i.e. The ASAM Criteria) to be a useful way to triage pain patients as well as addiction patients.
The most effective treatment for addiction often involves combining counseling with medication in a variety of settings based upon the severity and complexity of the individual’s disease state.
Similarly, the most effective treatment for chronic pain often involves combining physical therapy, supportive counseling, procedural interventions with medications in a variety of settings based upon the severity and complexity of the individual’s disease state.
So when I suggest that pain patients should be treated like addicts, I am not saying that pain patients are addicted. I am saying that both addicted patients and chronic pain patients can be treated effectively by utilizing The ASAM Criteria as a guide.
I hope that answers the “?”
A point I make repetitively on this subject, is the absolute necessity of saying what we mean. Where the truth is not accepted, it also won’t be told.
A fruitful area for future research, is the action of endorphins in complex pain syndromes.
We know very little about endorphin production, metabolism, and action. It appears that the opioid drugs, derived from poppy sap, have actions similar to endorphins.
We know that people whose endorphin production slows, as the result of major injury that confines them to a hospital bed, experience the same group of symptoms that are seen in opioid withdrawal.
Nobody wants to use the word, “addiction”, or even a milder word, like “dependency”, to explain normal people’s relationship to the endorphins secreted by their own bodies.
But if we removed the emotional charge and bellicose threats, that folks associate with those fighting words, and looked at this as a technical problem, we might surprise ourselves with what we learn about chronic pain syndromes.
In diabetes, it’s been known for decades, that an injury which renders inactive, a person whose pancreatic function was on the low end of normal, can cause diabetes to manifest itself. A slight reduction in insulin output, below normal, pushes the person over the edge, from normal, to diabetic, all because of an illness or injury.
Can the same thing happen to our endorphin output?
Is it possible that a triggering injury that knocks us into a hospital bed for several weeks, can set off a cascading chain of events, in which the endorphin system malfunctions, and pain becomes uncontrolled?
I can do no more than propose this as a hypothesis.
Nobody has done enough research into endorphin secretion, metabolism, and action, to offer more than guesswork.
Is endorphin-system dysfunction, a factor in opioid dependency that’s co-morbid with chronic pain?
Is endorphin-system dysfunction, a factor in crippling conditions like Complex Regional Pain Syndrome?
Do people who exhibit severe side-effects from even low-dose opioids (e.g. profound nausea and dehydration upon taking 5 milligrams of codeine), have abnormal endorphin secretion, metabolism, or reactions?
All reasonable questions, that nobody’s going to answer, until there’s some comprehension of what endorphins are and why they (usually) work.
If we waste all our time and energy, attempting to “prove” that people in pain, are imagining the pain, we’re not going to have time, energy, or money, to do any research that might actually save lives someday.
Which is why a little blunt candor is very refreshing. Thanks, Dr Murphy, for an enlightening post
I hope this is helpful…
Neuroadaptative mechanisms (sometimes called “neuroplasticity”) are believed to play a significant role in numerous brain processes (e.g. addiction, chronic pain). Endorphins – production, release and receptor activity – play a major role, but are only a portion of the whole picture. This is an exciting and promising area for research.
Here is a link to a nice summary article:
http://www.psychologytoday.com/blog/the-athletes-way/201403/is-impaired-neuroplasticity-linked-chronic-pain
And this entertaining YouTube video explains how one’s brain responds to chronic pain:
Thanks for commenting,
Dr Murphy
Loved the YouTube video. Dr. Murphy, I enjoyed your article. I am a chronic pain sufferer in need of a Pain Management Physician. I have been suffering from a “new” injury now since March of this year. My PCP is not helpful. I hope we may one day meet.
Fresh off the presses:
NIH PANEL
The Effectiveness and Risks of Long-Term Opioid Therapy for Chronic Pain: A Systematic Review for a National Institutes of Health Pathways to Prevention Workshop
Roger Chou, MD; Judith A. Turner, PhD; Emily B. Devine, PharmD, PhD, MBA; Ryan N. Hansen, PharmD, PhD; Sean D. Sullivan, PhD; Ian Blazina, MPH; Tracy Dana, MLS; Christina Bougatsos, MPH; and Richard A. Deyo, MD, MPH
Ann Intern Med. Published online 13 January 2015 doi:10.7326/M14-2559
http://annals.org/article.aspx?articleid=2089370
The Sumerians in Mesopotamia were among the first people identified to have cultivated the poppy plant around 3400 BC.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2711509
The Babylonians in Mesopotamia enacted a statute forbidding the dilution of beer with water, prescribing the death penalty for this offense.
Everyone who drank the Babylonians’ beer has since died.
And this proves exactly nothing about the efficacy or safety of ancient Babylonian beer.
Cause and effect is not the same as “associated with.” The sun rising each morning is associated with the rooster crowing. And for that matter, the sun does not “rise.” The earth turns relative to the sun. It all boils down to one’s perspective.
If you read the NIH article cited above, the authors employ liberal use of the term “associated with.” And my guess is that most of those authors do not suffer from chronic pain, otherwise they might have a different perspective.